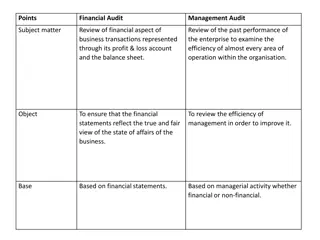
Audit of South London Intravenous Immunoglobulin Use: Comparing Dosing Methods
An audit conducted in South London comparing dosing methods for intravenous immunoglobulin use in clinical practice. Guidelines, calculations, and recommendations for dosing based on ideal body weight and adjusted body weight are discussed.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
An audit of South London intravenous An audit of South London intravenous immunoglobulin immunoglobulin use use in clinical practice: comparing dosing methods used in April comparing dosing methods used in April 2021 2021 in clinical practice: June 2021 Emily Crehan and Anna Wakelin Supervised by Professor Emma Baker, Professor of Clinical Pharmacology and South London IAP independent chair and Dr Drew Walker, clinical pharmacology fellow
Aims Aims Primary aims: Primary aims: To calculate potential Ig savings using the Ontario calculated dosing weight dose requested dose requestedin adults To calculate potential Ig savings using Ideal Body Weight in paediatric patients Ontario calculated dosing weightcompared to the Ideal Body Weight compared to dose requested dose requested Secondary aims Secondary aims: To compare approaches for rounding To compare different compare different dosing London Immunoglobulin Assessment Panel rounding the calculated dose to nearest vial size dosing methods methods to the dose requested for all referrals to the South
What do the guidelines say? What do the guidelines say? 1. For patients with BMI 30 kg/m2 or if actual weight >20% more than IBW, prescribers should consider using adjusted-bodyweight dosing of immunoglobulin. (Department of Health, July 2011) No firm recommendation for patients who don't fall into this category 2. Dosing (based on IBW) (NHS England and NHS Improvement, September 2019) 3. Ig prescribing will be based on ideal body weight- adjusted dosing (NHS England, November 2019) 4. In all paediatric patients IVIg dosing should be based on ideal body weight (IBW)... Where possible doses should be rounded down to the nearest vial size to prevent wastage. (NHS England, March 2020) 5. Dosing should be based on Dose-Determining Weight calculated as follows from the Ideal Body Weight: https://ivig.transfusionontario.org/dose/ (NHS England and NHS Improvement, May 2021)
How are these figures calculated? How are these figures calculated? Ideal Body Weight (IBW), Devine Formula is: Ideal Body Weight (male) = 50.0 kg + 2.3 kg (each inch > 5 feet) Ideal Body Weight (female) = 45.5 kg + 2.3 kg (each inch > 5 feet) Dosing Weight: is an adjusted body weight (of obese or overweight patients) and should only be used to calculate the dose of drugs for which there are recommendations specifying that the actual body weight should be adjusted for use in the dose calculations. Ontario calculated dosing weight Ontario calculated dosing weight = IBW + [0.4 x (Actual - IBW)] Exception: if Actual <IBW, then Dosing Weight = Actual
Evidence for Ontario dosing Evidence for Ontario dosing The latest NHS guidance advocates the use of ideal body weight- adjusted dosing (Ontario calculated dosing weight) based on evidence from two studies: Stump et al. (2017) compared the effectiveness of a precision-dosing strategy (IBW or Ontario calculated dosing weight), to actual body weight in patients with haematological malignancies. They found no significant difference in infection rates. Chow et al (2012) conducted an audit that demonstrated that implementation of the dosing weight calculator alone, resulted in a 6% decrease in the approved use of IVIG.
Who is being treated with IVIG? Who is being treated with IVIG? Total referrals for April 2021: 60* AVERAGE AGE (YEARS) AVERAGE WEIGHT (KG) 42 adult referrals: 34 with complete data, 8 with height not included Adult 55.3 (+/- 17.9) 73.6 (+/- 16.9) 18 paediatric referrals Paediatric 4.8 (+/-3.8) 21.0 (+/- 14.5) Total: 29 males, 31 females M:F ratio: 0.94 *2 additional patients were below the height where IBW could be used and were therefore excluded from our calculations.
What happened in April 2021? What happened in April 2021? Referrals Ig total dose requested (g) 3710 641 Ig saved compared to ABW dose (g) 407 30 Adults (42) Paediatrics (18) Total 4351 437
Adult dose saved using different methods Adult dose saved using different methods
Potential savings for adult patients using Ontario Potential savings for adult patients using Ontario and IBW dosing compared to doses requested IBW dosing compared to doses requested and Total dose requested = 3710g Average dose requested = 93g Using Ontario calculated dose (g) Additional patients that could be treated per month using Ontario calculated dose Using IBW dosing (g) Additional patients that could be treated per month using IBW dosing Total calculated doses 3683 - 3340 - Potential saving compared to dose requested 27 0.3 370 4.0 Potential saving compared to dose requested AND rounding down to nearest 5g vials 110 1.2 464 5.0 Potential saving compared to dose requested AND rounding down to nearest 10g vials 200 2.1 560 6.0
Paediatric Paediatric dose saved using different methods dose saved using different methods
Potential savings for paediatric patients Potential savings for paediatric patients using using IBW dosing compared to doses requested IBW dosing compared to doses requested Total dose requested= 641g Average dose requested=36g Pediatrics Using ideal body weight dose (g) Additional patients that could be treated per month using IBW dosing Total (g) 596 - Ig (g) potential saving compared to dose requested 45 1.3 Potential saving compared to dose requested AND rounding down to nearest 5g vials 81 2.3 Potential saving compared to dose requested AND rounding down to nearest 10g vials 111 3.1
Discussion Part 1 Discussion Part 1 Averages: it seems like Ontario calculated dosing is already being used as some hospitals use IBW and others use ABW. Confusion around dosing guidelines for adult patients: Of the 4 guidelines currently in use for adult dosing, there are 3 different approaches: 1. IBW for all patients 2. Ontario calculated dosing weight for all patients ( IBW-adjusted or dosing weight) 3. The use of Ontario calculated dosing weightonly when patients are obese (BMI >30 or ABW >20% of IBW) The Ontario calculator further suggests that if the ABW is below the IBW then the ABW should be used. Verbal reports from 7 South London trust representatives suggest there are 4 different approaches to dosing in practice: 1. IBW for all patients 2. Ontario calculated dosing weightonly when patients are obese (BMI >30 or high BMI ) 3. ABW with dose capped at 80kg 4. IBW for ICU patients and ABW for long-term patients with a dose cap at 90g
Discussion Part 2 Discussion Part 2 Rounding: There's inconsistency in guidelines (and practice) - should this be down to the nearest 5 or 10g? Paediatric patients: The guidelines are clearer, however, there is a need to clarify the method for calculating the IBW, as this is not currently stated in the guidelines and there are multiple potential methods. Emergency situations: concerns have been raised about the drawbacks of multi-step calculations. Lit review: no strong evidence for different methods Conclusions: There s an urgent need to clarify the dosing guidelines and to take a consistent approach across trusts. There s currently insufficient evidence to justify using IBW for all patients If it could be proven that it's safe to use an IBW approach and/or consistently rounding down 5g or 10g, additional patients could benefit from IVIG where IVIG availability is limited. Including dosing method and calculations in referrals would be very helpful for ensuring guidelines are being followed
References 1. Ameratunga R. Initial intravenous immunoglobulin doses should be based on adjusted body weight in obese patients with primary immunodeficiency disorders. Allergy Asthma Clin Immunol. 2017 Dec;13(1):47. 2. Anderson CR, Olson JA. Correlation of weight-based i.v. immune globulin doses with changes in serum immunoglobulin G levels. American Journal of Health-System Pharmacy. 2015 Feb 15;72(4):285 9. 5. Chow S, Salmasi G, Callum JL, Lin Y. Trimming the fat with an IVIG approval process. Transfusion and Apheresis Science. 2012 Jun;46(3):349 52. 6. Figgins BS, Aitken SL, Whited LK. Optimization of intravenous immune globulin use at a comprehensive cancer center. American Journal of Health-System Pharmacy. 2019 Nov 13;76(Supplement_4):S102 6. 7. Gajdos P. Treatment of Myasthenia Gravis Exacerbation With Intravenous Immunoglobulin: A Randomized Double-blind Clinical Trial. Arch Neurol. 2005 Nov 1;62(11):1689. 8. Grindeland JW, Grindeland CJ, Moen C, Leedahl ND, Leedahl DD. Outcomes Associated With Standardized Ideal Body Weight Dosing of Intravenous Immune Globulin in Hospitalized Patients: A Multicenter Study. Ann Pharmacother. 2020 Mar;54(3):205 12. 9. Khan S, Grimbacher B, Boecking C, Chee R, Allgar V, Holding S, et al. Serum Trough IgG level and Annual Intravenous Immunoglobulin Dose Are Not Related to Body Size in Patients on Regular Replacement Therapy. DML. 2011 Apr 1;5(2):132 6. 10. Koleba T, Ensom MHH. Pharmacokinetics of Intravenous Immunoglobulin: A Systematic Review. Pharmacotherapy. 2006 Jun;26(6):813 27. 11. Lagasse C, Hatton RC, Pyles E. A Survey of Intravenous Immune Globulin (IVIG) Dosing Strategies. Ann Pharmacother. 2015 Feb;49(2):254 7. 12. Muta H, Ishii M, Furui J, Nakamura Y, Matsuishi T. Risk factors associated with the need for additional intravenous gamma-globulin therapy for Kawasaki disease. Acta Paediatrica. 2006 Jan 1;95(2):189 93. 13. Rocchio MA, Hussey AP, Southard RA, Szumita PM. Impact of ideal body weight dosing for all inpatient i.v. immune globulin indications. American Journal of Health-System Pharmacy. 2013 May 1;70(9):751 2. 14. Rocchio MA, Schurr JW, Hussey AP, Szumita PM. Intravenous Immune Globulin Stewardship Program at a Tertiary Academic Medical Center. Ann Pharmacother. 2017 Feb;51(2):135 9. 15. Selcen D, Dabrowski ER, Michon AM, Nigro MA. High-dose intravenous immunoglobulin therapy in juvenile myasthenia gravis. Pediatric Neurology. 2000 Jan;22(1):40 3. 16. Stump SE, Schepers AJ, Jones AR, Alexander MD, Auten JJ. Comparison of Weight-Based Dosing Strategies for Intravenous Immunoglobulin in Patients with Hematologic Malignancies. Pharmacotherapy. 2017 Dec;37(12):1530 6. 17. Torbic H, Abdul-Wahab SS, Ennala S, Guduguntla N, Han X, Wang X, et al. Single-Center Experience of Outcomes and Prescribing Patterns of IV Immunoglobulin Use in Critically Ill Patients. Critical Care Explorations. 2021 Jan 11;3(1):e0314.