Biophysical Profile for Antepartum Fetal Assessment
Learn about the biophysical profile (BPP) test used for antepartum fetal evaluation, its parameters, indications, and physiological basis. Discover when to perform the test, its clinical utility, and the criteria for a non-stress test in BPP.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
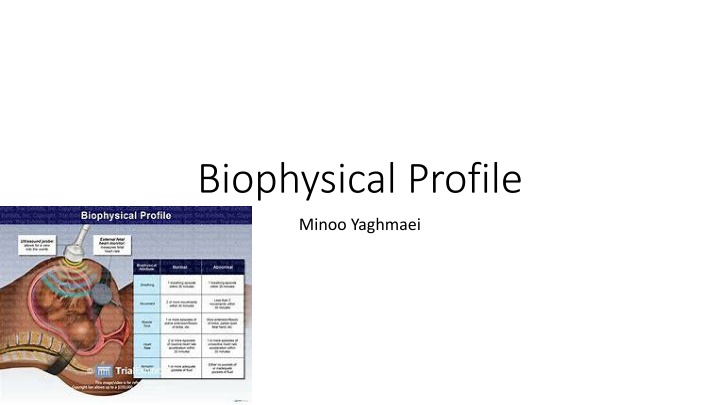
Biophysical Profile Minoo Yaghmaei
Biophysical profile test for antepartum fetal assessment Is a test performed antepartum for evaluating the fetus for signs of compromise Noninvasive Easily learned Easy performed
Biophysical parameters Fetal movement 0 2 Fetal tone 0 2 Fetal breathing 0 2 AF volume 0 2 NST 0 2 8 absence of significant CNS hypoxemia/ acidemia/ at the time of testing 4 can be a sign of fetal compromise In one study, BPP scores were higher if a test was performed in late evening compared with the morning
Indications: (ACOG) Preexisting or gestational diabetes treated with antihyperglycemic drugs Hypertensive disorders Fetal growth restriction Twin pregnancy Post term pregnancy Decreased fetal activity Systemic lupus erythematous Antiphospholipid syndrome Sickle cell disease Alloimmunization oligohydramnios or polyhydramnios Prior fetal demise PPROM Others: eg. Maternal vascular diseases, .
Possible indications Advanced maternal age Obesity Major fetal structural abnormalities Abnormalities in first and second trimester maternal biochemical Down syndrome screening results
BPP Antepartum Intrapartum: clinical utility is unclear ????
Physiologic basis of biophysical monitoring All biophysical activities are regulated and controlled by discrete centers in the brain, that are sensitive to both local factors and feed back from peripheral sensors Abnormal biophysical can be sign of hypoxemia, acidemia, ischemia Normal suppression of a regulatory center from intrinsic fetal rhythms like sleep or drugs Other biophysical activities like sucking
Criteria for BPP NST: reactive, at least 2 episodes of FHR accelerations, at least 15 BPM and at least 15 seconds- from onset to return associated with fetal movement Fetal breathing movements: 1 or more episodes of rhythmic breathing movements of 30 seconds within 30 minutes observation period Fetal tone: 1 or more episodes of extension of a fetal extremity or fetal spine with return to flexion Fetal movement: 3 or more discrete body or limb movements within 30 minutes of observation. An episode of active continued movement is counted as 1 movement AF: SPD 2 cm, the horizontal dimension should be at least 1 cm
BPP 4 of these parameters are acutely affected by fetal hypoxemia and acidemia. When one or more is normal, hypoxemia or acidemia can be reliably excluded. In contrast when 1 or more is abnormal, the possible causes need to be evaluated. It is unusual to observe absence of 2 or more acute parameters due to sleep alone More absent acute parameters and longer the absence of acute parameters Duration of sleep: 20 to 40 minutes
AF An AFI 5 cm and a DVP 2 cm is considered abnormal The American College of Obstetricians and Gynecologists concludes that DVP measurement, as opposed to AFI, is associated with fewer unnecessary interventions but comparable perinatal outcomes AF is a nonacute parameter since decrease in AF volume occur gradually, in response to redistribution of fetal blood flow in response to chronic uteroplacental vascular insufficiency
Duration of fetal observation Average time to obtain a normal BPP: 5.3 minutes, test can be stopped but can take up to 30 minutes To confirm a BPP is equivocal or worse: always require 30 minutes When all tests are considered the average time is 18 minutes The mean duration of a fetal sleep (no somatic movement) is 20 minutes Upper range of a fetal sleep is approximately 40 minutes NST with score 8/8 of BPP: dose not enhance the performance of BPP NST should be performed with score 6/8
interpretation 10/10 , 8/8 (without NST), 8/10 (including 2 points for AF) is a normal test result the risk of fetal death within 1 week is low (0.4 to 0.6 /1000 births) however a change in maternal condition affects this balance. fetal death after a normal BPP is often due to an unpredictable insult such as sudden cord prolapse , . 6/10 (including 2 points for AF) is a equivocal test result, as a significant possibility of developing fetal asphyxia can not be excluded a score of 6 was a poor predictor of an abnormal outcome the test is repeated within 24 hours
interpretation 6/10 or 8/10 with oligohydramnios (0 points for AF) is an abnormal test, and further assessment and correlation with the clinical setting are indicated risk of fetal asphyxia within one week is 89/1000 with expectant management these scores should be interpreted within the context of GA and maternal and obstetric factors and cervical state 0 /10 to 4/10 is abnormal, the risk of fetal asphyxia within 1 week is high if there is no intervention and delivery is usually indicated risk of fetal asphyxia within 1 week is 91 to 600/1000 delivery is usually indicated
Factors potentially affecting the score Antenatal corticosteroids can be associated with transient FHR and behavioral changes these changes typically return to baseline by day 4 after treatment the most change: decrease in variability on days 2 to 3 after administration, fetal breathing and body movements are also commonly reduced non reassuring fetal evaluation (NST or BPP)
Factors potentially affecting the score Subclinical infection the effect is controversial intra amniotic infection in a patient with PPROM may be associated with a low BPP score in the absence of hypoxemia most studies have not found the BPP score to be a very sensitive method for detecting subclinical infection
Factors potentially affecting the score Fasting point reductions during fasting were primarily due to nonreactive nonstress tests and inadequate movements Preterm labor May be associated with absence of fetal breathing movements
Factors potentially affecting the score Narcotics and sedatives can significantly lower the score
Evidence of efficacy Meta-analysis of randomized trials BPP vs. conventional FHR monitoring: did not reduce perinatal death or frequency of low Apgar scores Observational studies BPP is accurate for predicting the absence of significant fetal acidemia comparable to the OCT Physiologic data direct relationship between BPP score and mean umbilical venous PH BPP score accurately predicts both the probability and severity of existing acidemia relationship between BPP score and fetal PO2 is less precise
Testing schedule Initiation as soon as an increased risk of fetal demise is identified and delivery for perinatal benefit would be considered if test results are abnormal may be as early as 24 weeks of gestation 32 weeks of gestation has become a common threshold for initiation for fetal surveillance when an indication for fetal surveillance is present
Testing schedule frequency 10/10 or 8/10 without decreased AF: weekly or twice weekly until delivery until delivery when the high risk condition persists and appears stable
Route of delivery after a low BPP score false-normal test rate defined by an antepartum death of a structurally normal fetus that approximated 1 per 1000. the most common identifiable causes of fetal death after a normal BPP score include feto - maternal hemorrhage, umbilical cord accident, and placental abruption PPV of low BPP score: 50 % NPV: >99 % Mode of delivery based on : presentation, cervical findings, maternal condition In the absence of an obstetric contraindication: induction of labor with continuous intrapartum FHR monitoring
Modified BPP is abbreviated BPP required approximately 10 minutes to perform Modified BPP: AF & NST, the still birth within one week of a normal modified BPP is the same as with full BPP (o.8 per 1000). Since 90 % of women undergo a modified BPP will have a normal result, only a minority will need full biophysical evaluation. It saves time and money. False-negative rate of 0.8 per 1000 and a false positive rate of 1.5 percent. The American College of Obstetricians and Gynecologists has concluded that the BPP and modified BPP are comparable to other biophysical fetal surveillance approaches in predicting fetal well-being.




")