Candida Diaper Dermatitis in Infancy
Diaper dermatitis, particularly Candida diaper rash, is a common condition affecting infants, often linked to factors like stool irritation, antibiotic use, and infant skin physiology. Learn about its etiology, risk factors, and management strategies to address this prevalent dermatological issue in young children.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
CANDIDA DIAPER DERMATITIS [Diaper rash; Napkin dermatitis; Nappy rash] Dr. Immaculate Kariuki Consultant Paediatrician Nairobi, Kenya
Images in this presentation are intended for the education of clinicians only and may be upsetting to some viewers.
Case presentation A previously healthy 7 month old, baby T.B. presents with a diaper rash for the last 2 weeks that is not getting better. Initially the rash was raised and red; now it has erosions. Baby is irritable and fussy. The mother uses disposable diapers and has not changed the brand since birth. What further information will help you manage this child?
Further history oTW was introduced to solid food 1 month ago. o She had cough, fever & diarrhoea 1 week prior to developing the symptoms above which were treated with oral antibiotics for 5 days. o She also has mild facial eczema treated with emollients. Which factors above increase the likelihood of this baby getting diaper dermatitis? What things will you be looking for on the examination?
Introduction Diaper dermatitis (all causes) is the commonest dermatological condition in infancy (up to 1/5 of all dermatology visits in some series). Affects area covered by diaper - perineum, buttocks, inner thigh & abdomen sometimes. Peak 9 - 12 months. Persistent symptoms for more than 3 days likely due to an infectious component. Candida species are the commonest organisms associated with diaper dermatitis.
Etiology of Candida diaper dermatitis Candida albicans- most prevalent Rarer causes: C. tropicalis, C. glabrata, C. parapsilosis. Typically a superinfection of irritant dermatitis with Candida Candida species are present in <4% of diaper area without dermatitis
Risk Factors Irritation by stool, urine and diaper components Recurrent use of antibiotics Frequent stooling - a factor of age or diarrhoea. Immunosuppression Different infant skin physiology Dietary factors
Young infants skin function Skin microbiome is different, colonized primarily by Firmicutes, as opposed to Actinobacteria in adults. Breakdown products of filaggrin proteolysis, known as natural moisturization factor (NMF), is lower Newborn skin is drier with more trans-epidermal water loss (TEWL) initially as compared to older infants. Has smaller keratinocytes, denser microrelief structures thinner stratum corneum & epidermis. Diapered regions: skin hydration and skin pH is higher than rest of skin. The microbial flora colonizing buttocks area is similar to GI flora.
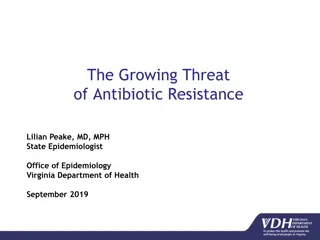
Pathogenesis Excessive moisture Friction Impaired skin barrier function Altered cutaneous microbiome Permeation by commensal candida. High enzymatic activity Increased PH
Diaper area irritation Redrawn from Pediatric Dermatology 2013;31 (1) :1-17
Increased PH Urease in stool breaks down urea in urine Bathing products PH imbalance Increased PH leads to increased enzyme activity Disrupted normal flora with higher risk of candidiasis
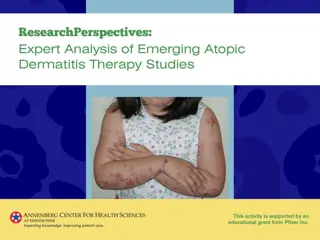
Clinical Presentation Irritability due to burning sensation and itching Persisting diaper dermatitis (more than 3 days) despite conservative treatment Characteristic rash involving the groin and gluteal folds Severe cases - erosion and ulceration.
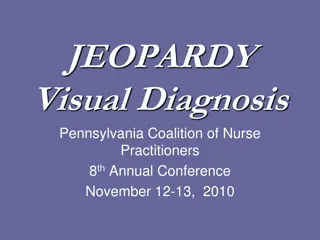
Candida diaper rash Raised edge, sharp margins with white scales, satellite papules and pustules - characteristic feature of Candida infection. Dutta et al Indian Pediatr 2015;52: 1100
Candida diaper dermatitis Red, erythematous & scaly plaques with maceration and edema on the perianal area, buttocks and inner thighs
Candida diaper dermatitis Red, erythematous & scaly plaques with maceration and edema on the perianal area, buttocks, lower abdomen, and inner thighs http://www.atlasdermatologico.com.br/disease.jsf?diseaseId=65
White scaly papules on folds http://www.atlasdermatologico.com.br/disease.jsf?diseaseId=65
Scaly & dry rash http://www.atlasdermatologico.com.br/disease.jsf?diseaseId=65
DIAGNOSIS Clinical Direct observation with KOH 10% shows pseudohyphae especially from the satellite lesions. Mycology culture
ABCDE ACRONYMN Effective for any-cause diaper dermatitis: Air Barrier Cleansing Diaper Education
What may alter management? Consider and look for bacterial superinfection. Look for oral candidiasis. Take a swab especially if bacterial infection suspected.
Topical Antifungals IMIDAZOLES - Clotrimazole, miconazole, ketoconazole and bifonazole - Applied twice a day for 7 10 day with high cure rates (50 to 68%) NYSTATIN - Commonly used. - Less effective than imidazoles. Switch if no response in 2-3 days CICLOPIROX - applied twice daily for 7 days. SERTACONAZOLE - fungicide with long skin durability (up to 72 h). - broad-spectrum third-generation applied twice daily for 14 days.
Oral antifungal agents Indicated for : - Concomitant GIT candidiasis, including oral - Severe cases Options - Fluconazole 3-6mg/kg /day - Nystatin 100,000 IU x 3-4 daily (not absorbed)
In addition to antifungals Remove the diaper - Eliminates the wet environment - Reduces contact between skin and stool & urine - Less irritation Consider steroids - Low potency for 1-2 weeks - Treat moderate to severe diaper dermatitis
If not resolving with conventional therapy? Underlying medical conditions: Type I diabetes Chronic mucocutaneous candidiasis Cow milk allergy Lactose intolerance Alternative diagnoses
Differential diagnoses Bacterial dermatitis mainly streptococcal & staphylococcal Psoriasis. Irritant contact dermatitis Exacerbations of seborrheic dermatitis or atopic dermatitis Scabies Nutrition deficiency especially zinc (acrodermatitis enteropathica) and rarely biotin deficiency
Streptococcal infection Bright erythema in the perianal region due to beta hemolytic Streptococci Bullae (tense, flaccid or eroded), pustules or vesicles may be present in impetigo
Psoriasis Well-demarcated bright red erythema in the diaper area due to inverse psoriasis (well demarcated, erythematous and glistening plaques with thin white scales, usually spares inguinal creases, involvement of the other body areas).
Irritant contact dermatitis Involves convex surfaces of inner thigh, lower abdomen, buttock, sparing intertriginous creases
Seborrhoeic dermatitis Look at the scalp.
Zinc deficiency Can be Inherited (acrodermatitis enteropathica-rare) or acquired. Presentation is similar when deficiency is severe perioroficial dermatitis Young infants are at higher risk of deficiency due to increased demand during growth. In young infants, dietary constraints such as delayed complimentary feeding and feeds high in phytate content also increase likelihood of defiency
Transcient Infantile Zinc deficiency Dassoni et al Dermatol ResPract2014;2014; 719701
Prevention Skin care practices that support skin barrier function and protect diaper area from urine & stool. Minimising diaper wear. Frequent diaper changes. Bathing at least daily in water with baby oil or water-dispersible creams. Cleansing gently. Barrier creams, ointments and pastes that are petrolatum based or contain zinc oxide, lanolin etc.
Does the type of diapers matter? Baer et al Disposable nappies for preventing napkin dermatitis in infants (data from 28 studies-upto 2003) Cochrane database syst Rev. 2006 Jul 19;(3):CD004262. There is not enough evidence from good quality randomised controlled trials to support or refute the use and type of disposable napkins for the prevention of napkin dermatitis in infants. The implications of this for practice are that health care workers, parents and infant caregivers are left to balance the many considerations in napkin choice without this evidence.
What about wipes or cleaning solutions? -Cleansing with wipes/water only -Bathing with water/ cleansing solution -Application of topical products Prevention of Diaper Dermatitis in Infants a Literature Review 2014. There seems to be no information on whether single skincare practices such as cleansing, bathing, and application of topical preparations can prevent DD. High-quality randomized clinical trials are needed to show the effectiveness of skin care practices for controlling & preventing DD. Blume-peytavi et al Pediatric Dermatology. 31; (4): 413-429
Summary Diaper dermatitis is a common skin condition of infancy Candida diaper dermatitis is the most frequent infection associated with diaper dermatitis Diagnosis is mainly clinical Prevention using proper diaper area skin care is KEY There is no type of diaper, cleansing agent, or barrier cream that has been found to be superior to others so far