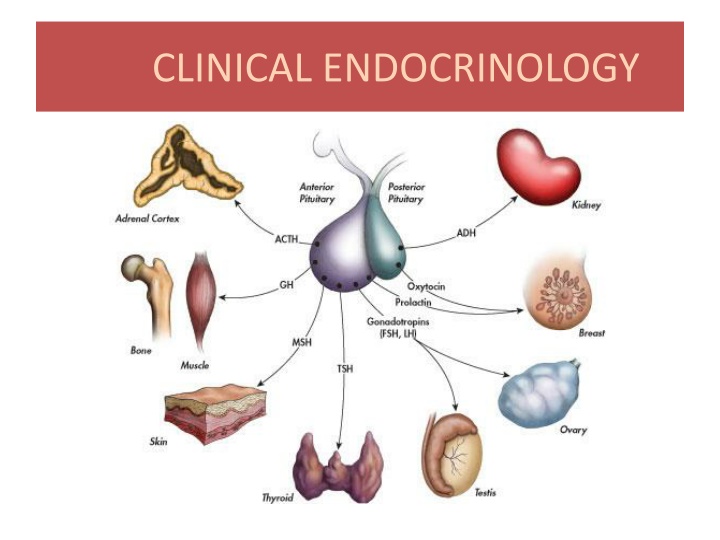
CLINICAL ENDOCRINOLOGY
The field of clinical endocrinology explores the intricate connection between the endocrine and nervous systems, delving into hormone regulation, gland functions, and hormonal disorders. Learn about the role of various glands, hormones, and their impacts on bodily functions.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
OBJECTIVES: 1. Explain why the endocrine system is so closely related to the nervous system. 2. Distinguish between an endocrine gland and an exocrine gland. 3. Define the term hormone and explain its general characteristics. 4. Distinguish between a steroidal and non-steroidal hormone, in terms of composition and action. 5. For each of the glands, name the hormone(s) they secrete, identify the target organ of each hormone, and the effect of each hormone. 6. Define the term gonadotropin, name of hormones secreted by the pituitary ,thyroid,adrenal glands,pancreatic gonadal gland . 7. Distinguish between dwarfism, giantism, and acromegaly 8. Describe how calcium levels are maintained in the blood. 9. The hormones that work together to regulate water and electrolyte levels in the blood and therefore regulate blood pressure. 10. Describe how glucose levels are maintained in the blood. 11. Compare and contrast cretinism, myxedema, Grave s Disease, and goiter. 12. Define the blood ,stimulatory tests, and other diagnostic procedures to define the disease. 13. To describe secondary sexual characteristics ,differentiate between virilism and hirsutism, get information about PCOS and ovulatory cycle. 14. Describe the adipose tissue -derived hormones ( leptin,adiponectin,resistin) and their role in adiposity
Learning outcomes 1. List the cells and state the hormones secreted by anterior and posterior pituitary,thyroid gland,adrenal,pancreas, gonads 2. Explain the role of hypothalamus in controlling anterior & posterior pituitary 3. Describe the regulation of secretion & actions of different hormones 4. Explain the neural control of hormone release. 5. Describe specific hormonal disorders 6. Describe the role of adipose tissue in regulation of body metabolism
Nervous and Endocrine Systems Act together to coordinate functions of all body systems Nervous system Nerve impulses/ Neurotransmitters Faster responses, briefer effects, acts on specific target Endocrine system Composed of endocrine glands that produce, store, and secrete hormones. HORMONE = a very powerful chemical substance secreted by an endocrine gland into the bloodstream, that affects the function of another cell or "target cell
Types of Glands Exocrine Glands are those which release their cellular secretions through a duct which empties to the outside or into the lumen (empty internal space) of an organ. These include certain sweat glands, salivary and pancreatic glands, and mammary glands. They are not considered a part of the endocrine system. Endocrine Glands are those glands which have no duct and release their secretions directly into the intercellular fluid or into the blood. The collection of endocrine glands makes up the endocrine system.The main endocrine glands are : pituitary (anterior and posterior lobes) thyroid, parathyroid - ` Adrenal (cortex and medulla) pancreas and gonads
Hormone types Circulating circulate in blood throughout body Local hormones act locally PARACRINE act on neighboring cells AUTOCRINE act on the same cell that secreted them
General characteristic of hormones 1. needed in very small amounts (potent); 2. produce long-lasting effects in the cells they target; 3. regulate metabolic processes (maintain homeostasis) 4. may be steroid (produced from cholesterol = fat-soluble) or non-steroid (water-soluble). 5. they have specific ratesand patterns of secretion (diurnal, pulsatile, cyclic patterns, pattern that depends on the level of circulating substrates) 6. they operate within feedback systems, either positive(rare) or negative, to maintain an optimal internal environment 7. they affect only cells with appropriate receptors specific cell function(s) is initiated 8. they are excreted by the kidney, deactivated by the liver or by other mechanisms
Some general effects of hormones Hormones regulate the transport of ions, substrates and metabolites across the cell membrane: 1. they stimulate transport of glucose and amino acids 2. they influence of ionic transport across the cell membrane 3. they influence of epithelial transporting mechanisms 4. they stimulate or inhibit of cellular enzymes 5. they influence the cells genetic information
Control of Hormone Secretion Control of secretion is in the form of neural, hormonal, or humoral stimuli. 1. Neural: Signals from nervous system The adrenal medulla is directly stimulated by the sympathetic nervous system. Epinephrine and NE reinforce the actions of the sympathetic nervous system. 2. Hormonal Occurs when hormones from one endocrine gland stimulate the secretion of hormones from another endocrine gland. E.g. TRH,TSH, TH E.g. CRH, ACTH,Cortisol These routes of secretion are usually controlled in a negative feedback manner. 3. Humoral : Chemical changes in the blood Occurs when substances other than hormones control the secretion of endocrine glands. E.g. Insulin secretion by the pancreas is determined by several factors. Rise in glucose after a meal triggers insulin secretion. Rise in amino acids after a meal triggers insulin secretion. In addition hormonal and neural stimuli also play a role in insulin secretion. or change in osmolarity (ADH release)
Chemical classes of hormones 1. Amino acid-derived: Hormones that are modified amino acids (catecholamines, thyroid hormones, prostaglandins, leucotrienes, dopamine, serotonine, GABA, melatonin) 2. Polypeptide and proteins: Hormones that are chains of amino acids of less than or more than about 100 amino acids, respectively. Some protein hormones are actually glycoproteins, containing glucose or other carbohydrate groups. (insulin, GH, Leptin...) 3. Steroids: Hormones that are lipids synthesized from cholesterol. Steroids are characterized by four interlocking carbohydrate rings.(a) Corticoids (cortisol, aldosterone,, b) sex hormones(androgen,estrogen, progesterone),c)Nitric oxide (NO) 4. Eicosanoids: Are lipids synthesized from the fatty acid chains of phospholipids found in plasma membrane. Hormones circulating in the blood diffuse into the interstitial fluids surrounding the cell. Cells with specific receptors for a hormone respond with an action that is appropriate for the cell. Because of the specificity of hormone and target cell, the effects produced by a single hormone may vary among different kinds of target cells.
Another groups of hormones A. gastrointestinal hormones (more than 26 GI polypeptides) B. opioid peptides (endogenic opioids) C. tissue growth factors (epidermal growth factor, nerve growth factor, PDGF, insuline-like growth factor ...) D. atrial natriuretic hormone (ANF) E. transforming growth factors and hematopoietic and other growth factors (FGF....) F. endothelial factors (endothelins, EDRF...) G. cytokines (interleukiny, interfer n, TNF....)
Hormones activate target cells by one of two methods, depending upon the chemical nature of the hormone. Lipid-soluble hormones (steroid hormones and hormones of the thyroid gland) diffuse through the cell membranes of target cells. The lipid-soluble hormone then binds to a receptor protein that, in turn, activates a DNA segment that turns on specific genes. The proteins produced as result of the transcription of the genes and subsequent translation of mRNA act as enzymes that regulate specific physiological cell activity. Lipid-soluble hormones are bound to plasma proteins and are less easily metabolized and excreted from the body. E.g. TH has a half-life of several days. E.g. Cortisol has a half-life of about 90 minutes
Blood capillary Blood capillary Blood capillary Free hormone Free hormone 1 Lipid-soluble 1 Lipid-soluble 1 Lipid-soluble hormone diffuses into cell diffuses into cell diffuses into cell diffuses into cell 1 Lipid-soluble hormone hormone hormone Transport protein Transport protein protein protein Transport Transport Lipid- soluble Activated receptor-hormone complex alters gene expression Activated receptor-hormone complex alters Activated receptor-hormone complex alters gene expression gene expression 2 2 2 Nucleus Nucleus Nucleus Receptor Receptor Receptor DNA DNA DNA Cytosol Cytosol Cytosol mRNA mRNA mRNA Newly formed mRNA directs synthesis of specific proteins on ribosomes Newly formed mRNA directs synthesis of specific proteins on ribosomes 3 3 Ribosome Ribosome New protein New proteins alter cell's activity 4 Target cell Target cell Target cell
Water-soluble hormones (polypeptide, protein, and most amino acid hormones) bind to a receptor protein on the plasma membrane of the cell. The receptor protein, in turn, stimulates the production of one of chemical messengers. - Water-soluble hormones are easily degraded by enzymes in the blood stream and are also excreted very quickly from the kidneys. E.g. insulin has a half-life of about 10 minutes in the body. E.g. Epinephrine has a half-life of about 10 seconds in the body.
Blood capillary Blood capillary Blood capillary Blood capillary Blood capillary 1 1 1 1 1 Binding of hormone (first messenger) Binding of hormone (first messenger) Binding of hormone (first messenger) Binding of hormone (first messenger) 1 Binding of hormone (first messenger) to its receptor activates G protein, which activates adenylate cyclase which activates adenylate cyclase which activates adenylate cyclase which activates adenylate cyclase which activates adenylate cyclase which activates adenylate cyclase Binding of hormone (first messenger) to its receptor activates G protein, to its receptor activates G protein, to its receptor activates G protein, to its receptor activates G protein, to its receptor activates G protein, Water-soluble hormone hormone hormone hormone hormone hormone Water-soluble Water-soluble Water-soluble Water-soluble Water-soluble Water- soluble Hormones Adenylate cyclase Adenylate cyclase Adenylate cyclase Adenylate cyclase Adenylate cyclase Adenylate cyclase Receptor Receptor Receptor Receptor Receptor Receptor Second messenger Second messenger Second messenger Second messenger Second messenger G protein G protein G protein G protein G protein G protein ATP ATP ATP ATP ATP 2 2 2 2 2 Activated adenylate cyclase converts ATP to cAMP ATP to cAMP ATP to cAMP ATP to cAMP Activated adenylate cyclase converts cyclase converts cyclase converts Activated adenylate Activated adenylate cAMP Activated adenylate cyclase converts ATP to cAMP cAMP cAMP cAMP cAMP 6 Phosphodiesterase inactivates cAMP Protein kinases Protein kinases Protein kinases Protein kinases cAMP serves as a second messenger to activate protein kinases kinases kinases kinases cAMP serves as a second messenger second messenger cAMP serves as a second messenger to activate protein to activate protein to activate protein cAMP serves as a 3 3 3 3 Activated Activated protein kinases kinases kinases Activated protein protein Activated protein kinases 4 4 4 Activated protein kinases phosphorylate cellular proteins cellular proteins Activated protein kinases phosphorylate Activated protein kinases phosphorylate cellular proteins Protein Protein Protein ATP ATP ATP ADP ADP ADP Protein Protein Protein P P P 5 5 Millions of phosphorylated proteins cause reactions that produce physiological responses produce physiological responses Millions of phosphorylated proteins cause reactions that Target cell Target cell Target cell Target cell Target cell
second messengers:The small molecule generated inside cells in response to binding of hormone or other mediator to cell surface receptors Calcium (Ca2+) Target: calmodulin Calmodulin protein kinases Cyclic nucleotides cAMP & cGMP Target: protein kinases Diacylglycerol (DAG) & IP3 Phosphoipase C act on the PIP2 From membrane lipids DAG Protein Kinase C (membrane) IP3 Ca2+ (triggers the release of Ca2+from the endoplasmic reticulum, which then activates enzymes that generate cellular changes.)
RECEPTORS: General Characteristics of Receptors Receptors bind hormones, resulting in a biological response All receptors exhibit general characteristics: 1. Specific Binding (structural and steric specificity) 2. High Affinity (at physiological concentrations) 3. Saturation (limited, finite # of binding sites) 4. Signal Transduction (early chem event must occur) 5. Cell Specificity (in accordance with target organ specificity).
All receptors have two functional domains: All receptors have two functional domains: 1. Recognition domain: it binds the hormone 2. Coupling domain: it generates a signal that couples the hormone recognition to some intracellular function. Coupling means signal transduction. Receptors are proteins. They are present in cell membranes Intracellular receptors: cytoplasmic receptors nuclear receptors
Cell Surface (membrane)Receptors Cell Surface (membrane)Receptors There are three types of cell surface receptors: 1. Ion channel receptors :Ionotropic 1. Transmembrane receptors: G-protein- coupled receptors,Metabotropic Receptors that are kinases or bind kinases: Protein kinases phosphorylation Neurotrophins
Cell surface receptors: G Cell surface receptors: G- - protein receptors A. Basic G-protein Receptor a. ligand binds to receptor (outer surface of cell). b. receptor changes shape (inner surface of cell). shape change allows receptor to bind inactive G-protein c. inactive G-protein binds to receptor d.receptor activates G-protein protein receptors
a. b. c. d. e. G-alpha drops GDP, picks up GTP when G-alpha binds GTP --> G-beta and G-gamma are released G-alpha + GTP is released from receptor into cytoplasm G-alpha + GTP = active G-protein. activated G-protein binds to target protein target protein's activity is altered - might be stimulated or might be inhibited . G-alpha + GTP is released from receptor into cytoplasm G-alpha + GTP = active G-protein. The G protein activates adenylate cyclase, the enzyme that catalyzes the production of cAMP from ATP.Cyclic AMP then triggers an enzyme that generates specific cellular changes - might be stimulated or might be inhibited . f. g. h. http://photos1.blogger.com/blogger/3716/526/400/G-receptor.jpg
Intracellular Receptors Some receptor proteins are intracellular, found in the cytosol or nucleus of target cells Small or hydrophobic chemical messengers (1st messenger,I,e hormone) can readily cross the membrane and activate receptors Examples of hydrophobic messengers are the steroid and thyroid hormones of animals An activated hormone-receptor complex can act as a transcription factor, turning on specific genes
The action of nuclear receptors is slow, as it takes some hours for the whole process to occur. The effect is long-lasting (or even permanent) and changes the properties of the cell. This type of process is important in development, differentiation and maturation of cells, e.g. gametes (eggs and sperm cells). Transcriptional activator proteins DNA RNA Proteins
Steroid Hormones Steroid Hormones Steroid hormones are lipid soluble. Steroids can diffuse through the membrane 1. Diffuse through the membrane 2. Binds & activates intracellular receptor. 3. Steroid-Receptor complex then enters the nucleus and binds to a particular sequence on the DNA which is called hormone response element (HRE). 4. Activates a gene. 5. Gene transcribed into messenger RNA. 6. mRNA goes to the ribosomes 7. Translate mRNA into protein
Thyroid and Retinoids go directly into the nucleus. Their receptor is already bound to HRE, but along with a co repressor protein which fails to activate transcription. The association of the ligand with the receptor results in the dissociation of the co repressor. Now this receptor- ligand complex can bind other co activator proteins and transcription begins.
Negative Feedback in the Hypothalamus. Most hormonal regulation by negative feedback Few examples of positive feedback hypothalamus maintains fairly constant levels of hormones because it operates The a negative feedback system. E.g: excitatory Hypothalamus Thyroid Stimulating Hormone-Releasing Hormone inhibitory Anterior pituitary Thyroid Stimulating Hormone Thyroid gland Thyroid hormones
positive feedback. In such a system, hormones cause a condition to intensify, rather than decrease. As the condition intensifies, hormone production increases. Such positive feedback is uncommon, but does occur during childbirth, where hormone levels build with increasingly intense labor contractions. Also in lactation, hormone levels increase in response to nursing, which causes an increase in milk production. The hormone produced by the hypothalamus causing the milk let down and uterine contraction is oxytocin.
A classic example is the production of estrogen in response to gonadotropins. The consequences (or the outcome ) of increased estrogen production are the further production of gonadotropins, thus promoting more estrogen production.
Mechanisms of hormonal alterations Endocrine diseases A. elevated hormones level Hormone excess Hormone deficiency Hormone resistance may be caused by: B. depressed hormones level 1. failure of feedback systems 2. dysfunction of endocrine gland or endocrine function of cells: a) secretory cells are unable to produce or do not obtain an adequate quantity of required hormone precursors b) secretory cells are unable to convert the precursors to the appropriate active form of hormon c) secretory cells may synthesize and release excessive amounts of hormone
3. degradation of hormones at an altered rate or they may be inactivated by antibodies before reaching the target cell 4. ectopic sources of hormones C. failure of the target cells to respond to hormone May be caused by: 1. receptor-associated disorders: a. decrease in the number of receptors hormone - receptor binding b. impaired receptor function sensitivity to the hormone c. antibodies against specific receptors d. unusual expression of receptor function 2. intracellular disorders:- a) inadequate synthesis of the second messengers b) number of intracellular receptors may be decreased or they may have altered affinity for hormones c) alterationsingeneration of new messenger RNA or absence of substrates for new protein synthesis
Primary & secondary endocrine diseases Based on site of hormone defect (either increase or decreased secretion), Endocrine disorders are classified as: A) Primary Disease: If defect is in the target gland from which hormone has originated B) Secondary Disease: If defect is in the Anterior Pituitary or Hypothalamus E.g., Primary hypothyroidism means decreased secretion of thyroid hormone from the Thyroid gland Secondary hypothyroidism means deficiency of Anterior pituitary/ Hypothalamic hormone which stimulates production of thyroid hormone from the thyroid gland (defect not in the thyroid gland)
Investigations for Endocine Disorders Basal hormonal concentrations 1. Basal plasma levels (one-time examination) 2. Diurnal dynamics of hormone concentrations (e.g. cortisol,growth H) 3. Other hormonal cycles (e.g. menstrual phase dynamics: cyclic changes of LH, FSH, estrogens and progesteron) 4. Urinary output: 24 hr Is alternative method for hormones with diurnal dynamics (cortisol, aldosterone) or pulsate secretion (catecholamines), 5. Hormonal metabolites - plasma, urine (e.g. C-peptide), 5- HIAA (hydroxyindole acetic acid),Serotonin metabolite Urinary excretion measurement in patients with suspicious carcinoid. I. 6. Indirect evaluation - measurement of a metabolic response (ADH ... diuresis, insulin ... glycaemia etc.)
II. Functional tests Functional tests:- 1. Inhibitory tests 2. Stimulatory tests Basal hormonal concentration very often doesn t allow to establish a diagnosis of hypo- or hyperfunction. Suspect hypofunction Stimulatory tests = quantification of functional reserve of endocrine gland, Insulin hypoglycemia test, Arginin infusion test,TRH test GnRH test,CRH test Suspect hyperfunction = quantification of responsibility of endocrine gland to inhibitory factors, e.g. Dexamethazone test, Dopaminergic drugs test Principles: negative feedback inhibition / stimulation direct stimulation / inhibition Inhibitory tests
Tumor markers in endocrinology Thyroglobulin (Tg), anti-Tg antibodies Markers of non-medullar thyroid carcinoma. CEA (carcinoembryonic antigen) Marker of non-medullar thyroid carcinoma (and ather malignancy e.g. colorectal ca) Diagnostic usage in combination with Tg and anti-Tg Ab Calcitonin, procalcitonin Hormonal product and diagnostic marker of medullar thyroid carcinoma (lower sensitivity that Tg for non-medullar thyroid ca) newborn screening : 1. Congenital hypothyroidism - incidence 1 : 5000 screening based on elevation of TSH 2. Congenital adrenal hyperplasia (CAH) - incidence 1 : 10-14000 screening based on elevation of 17-OH-progesterone 3. Phenylketonuria
Imaging methods Indications: A. Localization of endocrine active tumors, hyperplasia, ectopic hormonal production B. Evaluation of systemic complications 1. Native X-ray exams 2. Ultrasonography 3. CT / MRI 4. Scintigraphy 5. Angiography Biopsy Thyroid gland - unclear solitary nodule, tumors 2. Adrenal glands - rarely Thyroid gland - Fine needle aspiration biopsy (FNAB)



















Receptors")



















Related


Objective Structured Clinical Examination (OSCE): A Modern Approach to Assessing Clinical Competence



Dr. Zoidis Evangelos: Endocrinology & Metabolic Syndrome Expert at Agricultural University of Athens