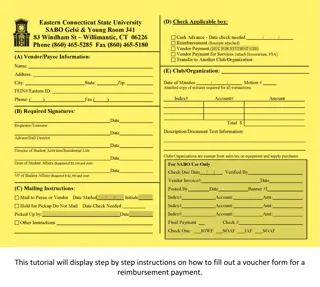
Drug Reimbursement Criteria and Evaluation Framework
Explore the principles of drug reimbursement, including the criteria for evaluating medicines' reimbursement, societal needs, safety, efficacy, and cost considerations. Learn how different countries assess and manage compulsory health insurance for drug reimbursement.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
RIZIV INAMI NIHDI pricing reimbursement Francis Arickx
National Institute for Health and Disability Insurance Social Security Manages Compulsory Health Insurance Stakeholders and Management
Reimbursement of Medicines The Basics - offer based, not demand driven - positive list nomenclature - (un)conditional reimbursement - temporary enlisting
For the evaluation of the systems, we used the accountability for reasonableness framework, developed by Daniels and Sabin. Accountability for reasonableness presumes that four conditions are fulfilled: 1. Transparency: the process must be fully transparent about the grounds for/rationales behind a decision. 2. Relevance: the decision must rest on reasons that all those affected by the decision can accept as relevant to meeting health needs fairly, given the resource constraints. 3. Revisability: decisions should be revisable in light of new evidence and arguments. 4. Enforcement/regulation: there must be some kind of regulation guaranteeing the three conditions described above.
Table: Key questions and possible criteria for a drug reimbursement appraisal process and examples of their operationalisation Medical, therapeutic and societal need Does the product target a medical, therapeutic and societal need? Medical need: - Life-threatening / non-life threatening condition - Severe / mild symptoms - Poor initial health state Therapeutic need: - Effective alternative treatments available / not available Societal need: - High / Low prevalence - Health inequality - Baseline health level - Medical need is operationalised and used in the decision process in the Netherlands and Sweden. Belgium in principle uses therapeutic need to define the cost sharing category, although in practice it seems that disease severity (independent from therapeutic alternatives) is the main consideration. Only France and Sweden assess(ed) the extent to which general needs criteria continue to apply over time by means of revisions of all reimbursed drugs. - Preparedness to pay out of public resources for a treatment Are we, as a society, in principle, prepared to pay for a treatment that will improve this indication out of public resources? - - Own responsibility Life-style related condition Only the Netherlands uses own risk and responsibility as formal appraisal criteria. All other countries apply the same criteria as for medical needs, indicating that these societies consider that treatments for high medical needs should be able to rely on public funding, independently from, for instance, patients life-style. Preparedness to pay out of public resources for the treatment under consideration Are we, as a society, prepared to pay for this particular treatment, given that we in general would be prepared to pay for a treatment for this indication? - Safety and efficacy of the treatment compared to the alternative treatment(s) Curative, symptomatic, preventive Therapeutic value Significance of health gains All countries explicitly evaluate the safety, efficacy and therapeutic value of drugs. Significance of health gains is a consideration for conditional reimbursement. - - Preparedness to pay more Given that we, as a society, are prepared to pay for this treatment out of public resources, are we prepared to pay more for this treatment than for the best alternative treatment? - - Added therapeutic value Potentially induced savings elsewhere in the health care sector Quality and uncertainty of the evidence Acceptability of co-payments and/or supplements Rarity of disease All countries consider added therapeutic value to be crucial for the preparedness to pay more for a drug than for its comparator. All countries use internal reference pricing to determine the reimbursement price of products with equivalent therapeutic value. Drugs classified as having added therapeutic value are more likely to obtain a higher reimbursement price (or -basis) in all countries - - - Willingness to pay (price and reimbursement basis) How much more are we willing to pay out of public resources for this particular treatment? - - - - - - Added therapeutic value Budget impact / ability to pay Cost-effectiveness ratio Medical, therapeutic and societal need Quality and uncertainty of evidence Limits to cost sharing (Added) therapeutic value (Added) therapeutic value is the most prominent decisioncriterion in all countries. The main focus is on safety, efficacy and effectiveness. France and Austria define several categories according to the degree of added therapeutic value; Belgium and the Netherlands only distinguish between added and equivalent therapeutic value. Sweden uses a continuous scale by directly linking the price to the level of added value. Budget impact Budget impact is considered in all countries. International price referencing is used in all countries but Sweden. This limits the effectiveness of countries price negotiations. All countries but France consider the incremental incremental costeffectiveness costeffectiveness ratio of a product but none defines an explicit threshold value (range). Countries are often unclear about how they handle uncertainty: it might affect either the value of the assessment elements, the reimbursement modalities or the final (conditional conditional) reimbursement decision. Cost sharing policies Cost sharing policies are implemented in all countries alongside social protection mechanisms. However, the accepted level of cost-sharing varies across countries. Belgium and France use the needs criterion to determine the level of cost- sharing for drugs; the other countries fully reimburse drugs but apply other costsharing policies.
Table: Key questions and possible criteria for a drug reimbursement appraisal process and examples of their operationalisation Medical, therapeutic and societal need Does the product target a medical, therapeutic and societal need? Preparedness to pay out of public resources for a treatment Are we, as a society, in principle, prepared to pay for a treatment that will improve this indication out of public resources? Preparedness to pay out of public resources for the treatment under consideration Are we, as a society, prepared to pay for this particular treatment, given that we in general would be prepared to pay for a treatment for this indication? Preparedness to pay more Given that we, as a society, are prepared to pay for this treatment out of public resources, are we prepared to pay more for this treatment than for the best alternative treatment? Willingness to pay (price and reimbursement basis) How much more are we willing to pay out of public resources for this particular treatment?
Reimbursement of Medicines The Process 3 step process - HTA - technical proposal - decision assessment appraisal Ministerial decision science, financing and politics
MARKETING AUTHORIZATION REIMBURSEMENT procedure reimbursement claim day 0 evaluation day 90 proposal day 150 decision day 180 ASSESSMENT APPRAISAL Commission for Reimbursement Minister Min ECONOM. AFF. procedure pricing
Reimbursement of Medicines The Theory Added Therapeutic Value Price Positioning Budget Impact Cost Efficiency
Negotiations are embedded in Negotiations are embedded in reimbursement legislation reimbursement legislation No separate process No separate process MARKETING AUTHORIZATION REIMBURSEMENT Managed Entry Procedure max. 120 days procedure reimbursement claim day 0 evaluation day 90 proposal day 150 decision day 180 Commission for Reimbursement Minister Min ECONOM. AFF. procedure pricing
A Managed Entry Agreement (MEA) is an arrangement between a manufacturer and payer/provider (coverage/reimbursement of) a health technology subject to specified conditions. that enables enables access access to These arrangements can use a variety of mechanisms uncertainty uncertainty about the performance performance of technologies or to manage the adoption of technologies in order to maximize their their budget budget impact impact. mechanisms to address address maximize effective effective their their use use, or limit limit Source: Int J Technol Assess Health Care. 2011 Jan;27(1):77-83.
MANAGED ENTRY AGREEMENTS Despite their proliferation, MEAs should not become a quick not become a quick- -fix solution fix solution to addressing the risk and uncertainty arising from the introduction of new therapies; instead, they should be integrated into a process integrated into a process of managed managed introduction of new therapies introduction of new therapies starting with horizon scanning horizon scanning and forecasting activities, proceeds to HTA assessment HTA assessment and continues with post post- - marketing studies and surveillance marketing studies and surveillance. Source: Panos Kanavos and Alessandra Ferrario. Managing Risk and Uncertainty in Health Technology Introduction: The Role of Managed Entry Agreements. Global Policy Volume 8 . Supplement 2 . March 2017
MANAGED ENTRY AGREEMENTS Key Features and components PERFORMANCE BASED COMPONENT VALUE/OUTCOME BASED COMPONENT MEA RISK SHARING COMPONENT
VALUE BASED COMPONENT (OUTCOME BASED ?) will determine the Willingness to Pay for an individual patient therapy Willingness to Pay for an individual patient therapy (in financial terms) which will depend on the added therapeutic value added therapeutic value of the therapy (as compared to the best alternative care), including the effect of the therapy on the QOL of Life) QOL (Quality will determine the Willingness to Pay on a societal level Willingness to Pay on a societal level which will also depend on the level of unmet medical need, and the subsequent priority setting priority setting (to invest in that given therapy) given the restrictions to allocate financial resources and budget limitations (overall budget impact, cost budget impact, cost- -efficiency,.. efficiency,..)
OUTCOME BASED COMPONENT ? performance based component ! will determine the Willingness to Pay for an individual patient therapy Willingness to Pay for an individual patient therapy (yes/no decision - gradient) which will depend on the clinical endpoints that clinical endpoints that are considered relevant determining the added therapeutic value of the therapy including the effect of the therapy on the QOL (Quality of Life) and on the capacity to establish these relevant endpoints and capture them in real life (Real World Data/Evidence Real World Data/Evidence) relevant for
RISK SHARING COMPONENT will determine the acceptance setting which will depend on the degree in which the assumptions/expectations of the effect of the therapy, based on the clinical trials evidence, will be met/confirmed by Real World Data/Evidence (as in real world, the therapy could perform better or worse than in a clinical trial setting) acceptance of the evidence from the clinical trials in a real life this component reflects the way in which uncertainties uncertainties are dealt with
Real World Evidence The Basics - offer based, not demand driven - positive list nomenclature - (un)conditional reimbursement - temporary enlisting Chapter IV: conditions on selected indications, duration, dosage, target population, required expertise,..
Conditional Reimbursement - Real World Evidence NHIDI refunding prescription authorization file patient request authorization physician health insurance documentary evidence prescription authorization prescription status insurance refunding authorization prescription pharmacist patient authorization status insurance medecines co-payment
Conditional Reimbursement - Real World Evidence NHIDI refunding prescription authorization file patient request authorization College Orphan Drugs physician health insurance documentary evidence prescription authorization prescription status insurance refunding authorization prescription pharmacist patient authorization status insurance medecines co-payment
Real World Evidence Conditional reimbursement is evolving from a mere control mechanism (quality and budget) towards collection of Real World Data / Evidence (?) in real and virtual registries
Real World Evidence the future is now electronic health record (patient and physician accountability) IT harvests disease registry Scientific Community processes Real World data (evidence ?) recommendations policy development/adjustment (alternative outcome based policy)
price.. what is on the price tag.. value..what s it worth.. cost.. of goods..
https://youtu.be/QUuFbrjvTGw KCE Academy RIZIV INAMI NIHDI pricing reimbursement - BeNeLuxA
Patient Public Politics Press Science..
Willingness to Pay Reluctancy to Refuse
Unmet Medical Need Expectations Uncertainties
Cost Budget Impact Efficiency Opportunity Cost
Economical Viability vs Shortages (COVID) Pricing International Price Referencing Profitability
Reference pricing system Ceiling Pricing Patent cliff Cheap Cheapest Biocliff Old Drugs Antibiotics
Monopoly Monopsony Payer Buyer
Pricing Budgeting Financing Mechanism
Balance: Pricing Budgeting - Financing PRICE REIMBURSEMENT LEVEL cost of goods R&D (re)investment bad reasons profits good reasons value (?) 33 PRICING BUDGETING
Reimbursement level.. reflection of.. good reasons.. willingness to pay (patient level) ..if confirmed performance risk sharing .. clinical trial evidence versus real life treatments willingness to pay (societal perspective) ..taking into account budget limitations/allocations, prioritization (Horizon Scan), preferences, sustainability ..capacity to finance on the long term bad reasons.. reluctance to say no (media / public pressure / emotions) 34 BUDGETING
BeNeLuxA in practice.. proof of concept for the coalition of the willing Main goal: To ensure access to innovative drugs at affordable cost Cooperation is part of the policy-mix Information gathering on global markets benefits from joint approach National context determines course of action Joint negotiations only in select cases What works? Setting clear, common goals Mutual benefit needs to be clear Pragmatic approach Focus on desired outcomes Lean organisational structure
BeNeLuxA in practice.. coalition of the willing on 4 domains Health Technology Assessment Horizon Scanning Exchange of information on pharmaceutical markets, prices and disease specific cross border registries Pricing and reimbursement including joint negotiation
BeNeLuxA in practice.. Information Sharing Drug consumption Prevalence and burden of disease Best practices in (health budget) management (e.g. hep. C approach, reference pricing, generic policy, biosimilar policy,..) Post marketing evidence gathering (e.g. registries) Policy questions (e.g. KCE-ZIN Study 2013-03-HSR_on drug pricing scenarios)
BeNeLuxA in practice.. Joint Health Technology Assessment Based on previous experience/expertise with MEDEV, EUnetHTA, JA2, informal collaboration,... Coherent and compatible with Joint Action 3 testing models for implementation: Mutual recognition of Assessments (operational) Joint writing /editing (operational) Sharing expertise (operational), eg. Dutch Wetenschappelijke AdviesRaad of ZIN acts as external expert in Belgian reimbursement procedure
BeNeLuxA in practice.. Pricing and Reimbursement, including joint negotiations By structural exchange of information and testing through pilots of procedures or scenarios for joint negotiations that lead to financial arrangements and contracts That are compatible with and respect national legislation and competence and responsibility of the different stakeholders in the decision making process That respect confidentiality of the commonly negotiated financial details (..nothing changes compared with today..) THIS IS NOT JOINT PROCUREMENT THIS IS NOT LIMBO DANCING.. how low can you go..
BeNeLuxA in practice.. Joined Horizon Scanning Prioritisation potential to improve access Allows for prioritisation of policy-making Allows for capacity planning for HTA bodies Allows for earlier planning for guidelines and registries Budget planning potential for savings Flags potential issues of displacement. Allows for better tools for budget allocation Efficiency gains potential to improve access Allows for streamlining procedures Level playing field potential for savings Allows for sharing earlier and lessening the current information asymmetry with industry Early dialogue strengthens collaboration Allows for stakeholders to share information at an earlier stage, e.g. Beneluxa Benefits Costs
BeNeLuxA in practice.. High impact reports Joined Horizon Scanning deliverables Dataset 1 (baselist) Filter Real time database Defined variables Dataset 2 (filtered list) Dataset 3 (high impact) High impact Withdrawn / failed pharmaceuticals Dataset 4 Registered pharmaceuticals Dataset 5 *AHRQ high impact report 2015 https://effectivehealthcare.ahrq.gov/sites/default/files/cancer-horizon-scan-high-impact-1512.pdf










 is an arrangement between a")


")