Early implementer site: Mental Health Inpatient
ELFT aims to increase smoking cessation rates among mental health inpatients through systematic identification, pharmacotherapy, behavioral support, and community follow-up. Data reflects high smoking prevalence and potential for improvement in support services. Strategies include quality improvement approaches and driver diagrams.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Early implementer site: Mental Health Inpatient Angela Bartley Consultant in Public Health & Deputy Director of Population Health
ELFT is an Early Implementor Site (EIS) 1. The NHS Long-Term Plan: smoking cessation to be provided for all inpatients, including in mental health. ELFT s aim: to increase the proportion of mental health inpatients to quit smoking either during their inpatient stay or following discharge in the community by October 2021 How? Implement Ottowa model by: systematic identification and documentation of all smokers admitted to a mental health ward; systematic administration of pharmacotherapy & behavioural support to active smokers admitted; systematic attachment to appropriate long term community follow-up after discharge: including from both specialist stop-smoking services, and support from CMHTs. Funding: 140k for 2020-21 available for TH, C&H and Newham 2. 3. 4.
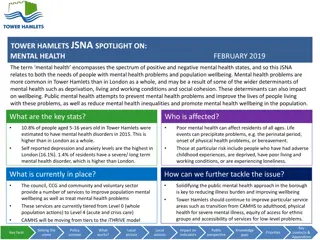
Taking a Quality Improvement Approach Taking a Quality Improvement Approach Data collection Very high proportions of ELFT s MH inpatients smoke: ranging between 49% (Bedford MH) and 57% (Newham and Hackney MH) Data collection High proportions of ELFT s service users receive very brief advice (VBA) about smoking reduction; smaller proportions receive referrals onwards to local stop smoking services. Variation between directorates suggests there could be room to improve the latter (left hand chart) Once discharged, MH former inpatients are not well engaged/supported by community stop smoking services. Data from Hackney shows that many of those referred by ELFT do not have sufficient contact details to be contacted; and SFH are unable to contact many others. Among those who are contacted, most do accept the service. Cascade diagram: outcomes for those referred to Smoke Free Hackney ELFT referrals vs all general referrals Smoke Free Hackney data via NRS; August 2019-July 2020 Proportions of inpatient smokers receiving VBA; or onward referral ELFT CQUIN data, 2019 Q1 - 2020 Q2 100% 120% Proportion of all referees who reach each point on 90% 100% 100% 100% 80% 97% 95% 70% 80% 79% 77% 74% 60% 65% 50% 60% 40% pathway 40% 30% 28% 20% 20% 19% 10% 0% 0% Total valid (non duplicate) referrals with sufficient contact details who live in area who SFH managed to contact who accepted service BD CH LT NH TH ELFT Directorate Proportion given VBA Proportion referred onwards via NRS Non-ELFT ELFT
Driver Diagram: Improving rates of smoking cessation after discharge from inpatient mental health setting AIM PRIMARY DRIVERS SECONDARY DRIVERS CHANGE IDEAS Trial a different referral protocol beyond NRS which doesn t routinely capture and include all relevant information Information flow to QuitRight Tower Hamlets Appropriate referral to community support Information on smoking cessation flow to CMHT Trial a smoking summary form to be agreed at CPA discharge meeting and then send to Quit Right Tower Hamlets and CMHT care coordinator Link between ELFT and QRTH to review referrals etc Integrated system Continue / strengthen regular review meetings between ELFT smoking cessation adviser and QRTH. Strengthen monitoring info for these meetings Increase the proportion of people discharged from MH inpatient setting who quit smoking (as measured 28 days post discharge), by 50%, by October 2021 Inform patient meaningfully of community support offer Trial three-way phone-based handover between the patient, smoking cessation adviser (ELFT) Support to access community support (at daunting time) Community MH Stop Smoking Advisors are ELFT Staff and in CMH teams Trial virtual (video) smoking cessation support provided by QRTH alongside CMHT support (i.e. patient attends (familiar) CMHT sites and accesses QRTH via videolink) Encouragement and very brief advice from CMHT care coordinator Support from CMHT/ Peer Support Workers Use successful peer support worker model for smoking trial peer support worker to make stopping smoking part of your recovery journey CMHT staff trained and confident to provide smoking cessation advice? trial providing VBA or level 2 training for CMHT staff and physical health workers Staff knowledge and skills provide clearer information for CMHT staff on different services available, how to refer, etc. CMHT staff have knowledge of available SSS services
Tobacco Dependency Pathway review Tobacco Dependency Pathway review 2. NRT should be made available as a regular medication for all smokers; Nurses should be able to prescribe regular combination NRT 3. All those who are undertaking abstinence with support should be encouraged to attempt sustained quit while inpatient 1. All patients who smoke should be flagged and receive specialist cessation support while they are inpatient Referral on opt-out basis to all smokers Support from specialist tobacco dependency advisor as an inpatient planning for smoke free discharge / e cigarettes This is in line with best practice and crucial to preventing harmful withdrawal symptoms. Tobacco dependency advisors to work up to setting quit date If not quitting / harm reduction as inpatient to be offered support to plan smoke free discharge 4. E-Cigarettes should be offered to smokers who wish to use them, as a second-choice alternative to NRT Post-discharge support 5. Improve monitoring across the pathway E-cigs to be offered as second-choice alternative, for those who refuse NRT. This should include monitoring the proportion of smokers identified; offered VBA; seen by a smoking cessation specialist; who set a quit date; and who are referred to specialist services on discharge. QI programmes across East London Directorates to develop and test change ideas. Move to community MH team with stop smoking advisor as part of your discharge package Link to peer support worker / programme
Engagement of Clinical Teams Data Flow Total re think of the data collection process and data flow Engagement and priority during a pandemic Discussion on the inpatient environment being a good place and time to quit Complexity across smoking systems & follow up by borough smoking teams complex Learning Evidence of effectiveness Logistics Ottawa model in a MH Inpatient setting Funding release and confirmation Using a QI Methodology to engage staff Debate over KPI s and data returns COVID

")