Malnutrition results from inadequate nutrition intake, leading to physical and mental decline. Learn about the causes, indications, routes of intervention, and available enteral nutrition products for addressing malnutrition in patients.
Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
Definition of Malnutrition Malnutrition can be defined as a state resulting from lack of intake or uptake of nutrition that leads to altered body composition (decreased fat free mass) and body cell mass leading to diminished physical and mental function and impaired clinical outcome from disease Cederholm T, et al., ESPEN guidelines on definitions and terminology of clinical nutrition, Clinical Nutrition (2016)
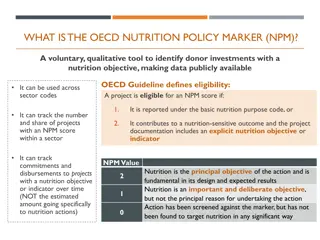
Etiology of Malnutrition The Academy of Nutrition and Dietetics/The American Society for Parenteral and Enteral Nutrition Consensus Malnutrition Characteristics: Application in Practice; Nutr Clin Pract. 2013;28:639-650
Indication EN If under nutrition already exist nutritionally problems Unintentional weight loss Insufficient to meet requirement to metabolic demand If it is anticipated that the patient will be unable to eat more than requirement If an inadequate food intake ( < 80 % of estimated energy expenditure) is anticipated for more than requirement
Route of Enteral Nutrition Protein and energy enriched Oral Sip feeding Naso gastric* Pharyngostomy Percutaneous endoscopic gastromy (PEG) or G-tube (button) Gastric Oesophagostomy Enteral Nutrition Radiological Inserted gastronomy (RIG)* Gastronomy* Surgical gastronomy Nasoduodenal* Tube Feeding Duodenal Extended gastronomy* Naso jejunal Extended gastronomy* Jejunal Direct access Surgical jejunostomy Fine needle catheter
Enteral Nutrition Products KALBE NUTRITIONAL PRODUCTS NUTRISI PARENTERAL NUTRISI ENTERAL GANGGUAN GINJAL GANGGUAN HATI TINGGI PROTEIN NEUROLOGI SISTEM IMUN KANKER SEIMBANG ANAK HEPATOSOL/ HEPATOSOL LOLA NEPHRISOL/ NEPHRISOL-D PEPTIBREN PEPTIMUNE ENTRAMIX NUTRICAN PEPTISOL ENTRAKID
Indication PN If early EN is not feasible or available over the first 7 days after admission. More than 10% involuntary weight loss over a 2-3 months period. Less than 75% of ideal or usual body weight Serum prealbumin less than 10 mg/dl serum transferrin less than 100 mg/dl History of inadequate oral intake for more than 7 days .
Route of PN > 900 mOsm/L Amino acid > 5 % Dextrose > 20 % Lipids Includes vitamins, minerals, and trace elements PN for > 7 14 days 600 900 mOsm/L PN for short-term < 7 14 days
Complications PN Metabolic Overfeeding Gastrointestinal Hyperglycemia Electrolyte imbalance Prerenal azotemia Abnormal acid- basa balance Hepatic steatosis Hyperglycemia Prerenal azotemia Increased CO2 production Respiratory distress syndrome Liver function disorder Gastrointestinal atropy
Monitoring PN Glucose Fluid and electrolyte balance Renal and hepatic function Triglycerides and cholesterol Body weight Nitrogen balance Plasma protein Creatinine/height index
Guidelines for Nutritional Monitoring Test Initial Stable Hospitalized Patient Home Patient Body weight Output : urin stool Urine glucose Blood : Glucose Electrolytes BUN, creatinine Total protein, Albumin transferrin Calcium, phoshorus LDH, AST, Bilirubin Alkaline phosphatase TIBC,iron CBC, differential, prothrombin time Anthropometrics Nitrogen balance daily every 8 hours every 6 hours daily daily daily every 6 hours twice weekly twice weekly twice weekly twice weekly daily daily daily weekly every other day every other day weekly weekly weekly monthly monthly monthly weekly weekly monthly weekly weekly monthly Weekly weekly weekly weekly monthly monthly twice weekly monthly weekly monthly monthly











")