This trial aims to assess the clinical and cost-effectiveness of intravenous sodium bicarbonate in critically ill adults with metabolic acidosis and AKI. The study involves a pragmatic multi-centre RCT with a sample size of 2,250 patients, focusing on 90-day all-cause mortality and cost-effectiveness outcomes. Primary and secondary outcomes include mortality, organ support duration, hospital stays, and quality of life assessments. Recruitment is set from April 2022 to August 2026.
Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
www.icnarc.org Multicentre evaluation Of Sodium bicarbonate in Acute kidney Injury in Critical Care Training for Screening & Randomisation IRAS: EudraCT: 2021-002587-44 REC Ref: 21/NW/0228 Sponsor: UHDB/2021/027 1003836 NIHR CPMS ID: 49697 ISRCTN Registry: ISRCTN14027629 Funding: NIHR HTA 129617 Chief Investigators: Prof Lui Forni & Prof Nick Selby
Agenda Trial overview and aim Screening Randomisation www.icnarc.org 2
Aim To evaluate the clinical and cost-effectiveness of intravenous sodium bicarbonate, 8.4% w/v www.icnarc.org Research question Population Intervention Comparator Outcome In critically ill adults with metabolic acidosis & AKI is IV sodium bicarbonate, 8.4% w/v superior to no IV sodium bicarbonate in terms of - All-cause mortality at 90 days - Incremental costs, QALYs and net monetary benefit at 90 days 3
Trial design Pragmatic multi-centre, open, data-enabled RCT o with internal pilot phase and integrated economic evaluation www.icnarc.org Sample size: 2,250 patients (randomised 1:1) Setting: 70 NHS adult critical care units Recruitment period: April 2022 end of August 2026 4
Outcomes Primary o 90-day all-cause mortality (clinical effectiveness) o Incremental costs, quality-adjusted life years and net monetary benefit at 90 days (cost-effectiveness) www.icnarc.org 5
Outcomes Secondary o Mortality at critical care unit discharge, 28 days and one year www.icnarc.org o Receipt and duration of respiratory, renal, and advanced cardiovascular organ support during the critical care stay o Duration of critical care unit and acute hospital stay o At 90 days and one year: On-going requirement for KRT Health-related quality of life Resource use and costs o Estimated lifetime incremental cost-effectiveness 6
Agenda Trial overview and aim Screening Randomisation www.icnarc.org 7
Patient flow diagram Screening Randomisation Safety monitoring Data collection IV sodium No sodium bicarbonate bicarbonate, 8.4% w/v Consent Follow-up 8
Inclusion criteria Patients admitted to critical care units fulfilling the below, at any point during the critical care unit stay: 1. Adult (aged 18 years) 2. Metabolic acidosis (arterial blood gas values of pH <7.30 and PaCO2 <6.5 kPa) 3. AKI KDIGO stage 2 or 3, defined as any one of the following three criteria: Serum creatinine 2.0 times baseline or Serum creatinine 354 mol/L, AND either a rise of 27 mol/L within 48 hours or serum creatinine 1.5 times baseline or Urine output of <0.5 ml/kg/h for 12 hours 9
Baseline serum creatinine value If available, use pre-hospitalisation value within 365 days of current hospital admission date If multiple pre-hospitalisation values, use the one closest to the date of current hospital admission If a pre-hospitalisation value from the 365 days prior to admission date is not available and there are multiple values from the current hospitalisation prior to the onset of the acute illness, then use the lowest one from the current hospitalisation If no baseline value is available, then estimate it using the provided calculator (see next slide) www.icnarc.org 10
Baseline serum creatinine - calculator www.icnarc.org Estimated baseline serum creatinine will appear in column F Enter patient s age and sex (1=Male, 2=Female) 11
Exclusion criteria (Protocol v4.0) If corrected, patient may be reconsidered for trial 10. Symptomatic hypocalcaemia (Ionised calcium <1.05 mmol/L)* 11. Hypernatraemia (Plasma sodium >150 mmol/L)* 12. Severe hypokalaemia (Potassium <3.0 mmol/L)* 13.Death perceived as imminent 14. Known hypersensitivity to IMP or excipients 15. Previously randomised into MOSAICC 1. Respiratory acidosis (acute or chronic) 2. KRT planned to start within 3 hours and treating clinician(s) unwilling to defer if randomised to sodium bicarbonate 3. Deemed unsuitable for KRT 4. High output stoma/ileostomy 5. Percutaneous biliary drainage 6. End stage kidney failure defined as documented eGFR<15 ml/min/1.73m2 prior to onset of this acute illness or end stage kidney disease (ESKD) on dialysis 7. Known renal tubular acidosis 8. Diabetic ketoacidosis 9. High anion gap acid poisoning (e.g. PEG, aspirin, methanol) Intended to exclude those with pre-existing kidney failure or on long-term chronic dialysis 12
FAQs Specified time limit between meeting eligibility and randomisation? o No, but please randomise ASAP once eligibility has been confirmed o Patients should meet all inclusion criteria and no exclusion criteria at the point of randomisation www.icnarc.org Who can confirm eligibility? o A doctor, medical practitioner or nurse as long as appropriately qualified, have undergone study training (documented on Training Log) and signed off on the Delegation Log GCP training not required o Must still be overall oversight by a medically qualified doctor 13
Co-enrolment Observational studies (including those collecting samples) o Permitted without prior agreement www.icnarc.org Interventional studies o Decided case-by-case by TMG o Co-enrolment acceptable with: ABBRUPT ADAPT-SEPSIS A-STOP AIRWAYS-3 ABC POST ICU EMERALD MARCH GENOMICC HARMONICS IRehab PRONTO RECOVERY SHORTER T4P TRAITS UK-ROX VITDALIZE 14
Agenda Trial overview and aim Screening Randomisation www.icnarc.org 15
Patient flow diagram Screening Randomisation Safety monitoring Data collection IV sodium No sodium bicarbonate bicarbonate, 8.4% w/v Consent Follow-up 16
Randomisation 24/7 web randomisation service o Can use generic/group or individual email addresses o Confirm local account with your local research team o Email mosaicc@icnarc.org to set up account(s) and notifications www.icnarc.org Who can randomise? o Signed off on Training and Delegation Logs o GCP training not required Randomisation Form o A hard copy must be completed and signed off for each patient at the point of randomisation 17
To consider www.icnarc.org 8.4% Sodium bicarbonate given centrally or peripherally? Follow local policy but depending on this Sodium bicarbonate may need to be administered centrally Therefore, if the patient is otherwise eligible but does not have central access and there are no plans for it for their care (and the IMP should be given centrally), then do not randomise the patient. Record this patient as Eligible not randomised and document the reason on the screening log 19
Remember www.icnarc.org All ABG values on the randomisation form should be from the same ABG This ABG must be the most recent ABG prior to randomisation 20
Possible randomisations SODIUM BICARBONATE (INTERVENTION) o Give sodium bicarbonate according to trial protocol (flowchart), do not commence kidney replacement therapy (KRT) o Please refer to Intervention Flowchart www.icnarc.org NO SODIUM BICARBONATE (CONTROL) o Do not give sodium bicarbonate o Continue with usual care, may include KRT at the discretion of the treating clinician. 21
Local communication COMMUNICATE the treatment allocation to bedside staff Prescribe as appropriate Ensure appropriate treatment Document in medical notes Leave documents at bedside e.g. intervention flowchart bedside notices adapt for your site www.icnarc.org 22
Intervention period Begins immediately following randomisation www.icnarc.org Intervention will continue until discharge from critical care, initiation of KRT or 90 days, whichever comes first o If patient is discharged and readmitted to ICU, treatment will be at the discretion of clinical staff 23
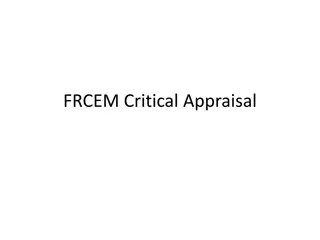
Sodium bicarbonate, intravenous 8.4% w/v Aiming to restore pH to 7.30 Any brand with marketing authorisation in the UK may be used Trial-specific labelling is not required Dispensed in accordance with a prescription (prn up to a max daily dose of 500ml/24 hours) www.icnarc.org Dosage schedule 50 ml administered over 30-60 minutes Maximum daily dose 500 ml / 24 hours Arterial blood gas should be performed 1-2 hours after each infusion 24
Intervention Flowchart Randomisation IV 8.4% w/v sodium bicarbonate* No sodium bicarbonate* Repeat sodium bicarbonate infusion, up to a max daily dose of 500ml/24hrs* ABG 1-2 hrs post-infusion pH < 7.30 pH 7.30 Monitor pH for duration of critical care unit stay, initiation of KRT or 90 days, whichever comes first pH < 7.30 pH 7.30 25
www.icnarc.org Respiratory acidosis Where the pH remains <7.3 and the PaCO2 has risen to 6.5 then consider a respiratory component to the acidosis The base excess may also support this diagnosis If respiratory acidosis is contributing to the low pH then this would be an acceptable reason for not giving sodium bicarbonate Discuss with the clinical team, to decide whether it is appropriate to administer sodium bicarbonate If not administered, this will be captured on a deviation form on the CRF.
No sodium bicarbonate Do not give sodium bicarbonate o If patient receives it, this is considered a protocol deviation o Research team will be expected to document concentration, volume and date received www.icnarc.org Continue with usual care, may include KRT at the discretion of the treating clinician 27
Kidney Replacement Therapy (KRT) *Indications to commence KRT may develop following randomisation (in either group) Initiation is at the discretion of the treating clinician As a guide, KRT may be considered where at least two of the following criteria are present: o Urine output <0.3 mL/kg/h for at least 24 hours o Arterial pH <7.25 despite adequate volume resuscitation, or in the intervention group an arterial pH <7.25 after adequate administration of sodium bicarbonate (defined as sodium bicarbonate treatment for 24 hours or administration of the maximum 500ml/24 hours, as per algorithm) o Hyperkalaemia (serum potassium >6.5 mmol/L) o Fluid overload intractable to diuretics www.icnarc.org 28
Staff awareness Ensure staff are aware of trial and intervention flowchart o Including temporary/bank/agency staff Ensure clear documentation of prescription/dosing and proper handover to subsequent shifts Discussion point at ward rounds Use stickers/labels/signs www.icnarc.org 29
Patient flow diagram Screening Randomisation Safety monitoring Data collection IV sodium No sodium bicarbonate bicarbonate, 8.4% w/v Consent Follow-up 30
Consent Patients may lack capacity at time of randomisation www.icnarc.org MOSAICC has ethics approval for deferred consent or researchwithout prior consent o Eligible patients may be recruited without prior consent After randomisation and once patient s medical situation is no longer considered an emergency, consent procedures should begin o Must be carried out by a GCP-trained team member o Personal Legal Representative should be approached first if patient still lacks capacity 31
Patient flow diagram Screening Randomisation Safety monitoring Data collection IV sodium No sodium bicarbonate bicarbonate, 8.4% w/v Consent Follow-up 32
Safety monitoring www.icnarc.org If you consider there are any adverse events or reactions, please discuss with the PI/research team For example: - Alkalosis (ABG value of pH 7.55) - Hypokalaemia (Potassium <3.2 mmol/L) - Hypernatraemia (Plasma sodium >150 mmol/L) - Hyperosmolarity (Serum osmolarity >300 mOsm/L) - Hypocalcaemia (Ionised calcium <1.05 mmol/L) - Hypoglycaemia (Blood glucose <3.5 mmol/L) - Deterioration of hemodynamic status associated with volume overload - Extravasation - Tissue necrosis caused by incorrect administration (intra-arterial, paravenous) 33
Randomisation Errors o Once randomised, patient is in trial and included in the analysis (unless a duplicate) Patient should continue with the randomised treatment (unless deemed clinically inappropriate) Consent and data collection must be carried out per protocol www.icnarc.org o If patient accidentally randomised twice, use first randomisation Check email notification if unsure (or contact local team/ICNARC CTU) Do not re-use the second randomisation details 35
FAQs What if a patient has received sodium bicarbonate prior to randomisation? o This is not an exclusion. If they still meet eligibility criteria, they can be randomised o Record volume of sodium bicarbonate received in the 24 hours prior to randomisation in the CRF www.icnarc.org Specified time limit between randomisation and first dose of sodium bicarbonate? o No, but first dose should be given ASAP after randomisation 36
FAQs IMP given centrally or peripherally? www.icnarc.org o Ultimately depends on your Trust guidelines but the investigators agree 8.4% w/v sodium bicarbonate would usually be given centrally, though a dose in an emergency could initially be delivered peripherally o If the patient is otherwise eligible but does not have central access and no plans for it for their care, then record this patient as Eligible not randomised and document the reason on the screening and enrolment log 37
FAQs Do prescribers need to be GCP trained if they are only going to prescribe? www.icnarc.org o If prescribing is part of their job, they will not require GCP o However, they will have to have undergone training in the study protocol and procedures and be signed off on the Training Log 38
Thank you! Any questions? www.icnarc.org Local research team PI: [XXXXX] Lead research nurse: [XXXXX] [any other local details] 39
https://www.icnarc.org/Our-Research/Studies/Current- Studies/MOSAICC/home Lead Investigators ICNARC CTU Team Catherine Oversby (Trial Manager) Lizzy Iroajanma (Research Assistant) Julie Camsooksai (Clinical Research Assistant) Carly Au (Senior Data Manager) Julia Edwards (Trial Statistician) James Doidge (Senior Statistician) Doug Gould (Senior Researcher) Paul Mouncey (Head of Research) Sponsor Representative Kate Threapleton (Clinical Trials Manager) Lui Forni (Chief Investigator) Nick Selby (Chief Investigator) James Doidge (Senior Statistician) Doug Gould (Senior Researcher) David Harrison (Head Statistician) Luke Hodgson (Consultant) Kathy Rowan (CTU Director) Zia Sadique (Health Economist) Manu Shankar-Hari (Professor) Michael Wise (Patient representative) Kelly Wright (Lead AKI Nurse) 40













")















")