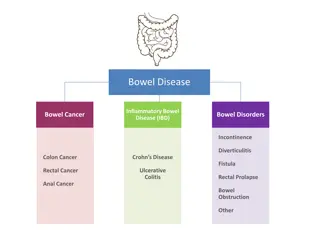
Extraintestinal Manifestations of Inflammatory Bowel Disease

Inflammatory Bowel Disease (IBD) presents various extraintestinal manifestations beyond the digestive tract. Learn about common and uncommon manifestations, when urgent treatment is needed, treatment options, and associated complications. Explore the immune-mediated conditions like Crohn's disease and ulcerative colitis, symptoms, complications, and disease prevalence in the US population.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Common and Uncommon Extraintestinal Manifestations of Inflammatory Bowel Disease Robert W. Isfort, MD
Disclosures Takeda Pharmaceuticals- Speakers Bureau Bristol Meyers Squibb- Speakers Bureau Chapter President, Crohn s and Colitis Foundation of Southern Ohio
Learning Objectives Review inflammatory bowel disease (IBD) pathogenesis, presentation, and epidemiology in relationship to extraintestinal manifestations Review common and uncommon manifestations of IBD outside of the intestines Identify when urgent treatment or referral is needed for extraintestinal manifestations Discuss treatment options for extraintestinal manifestations Review extraintestinal complications of IBD
Inflammatory Bowel Disease Immune mediated inflammatory diseases characterized by chronic inflammation of the digestive tract Crohn s disease Ulcerative colitis Microscopic colitis Segmental colitis associated with diverticulosis Symptoms Diarrhea, abdominal pain, tenesmus, hematochezia, weight loss, fever, vitamin and mineral deficiencies, failure to thrive, EIMs Emergent complications: Bowel obstruction Fistula/abscess Toxic megacolon Severe bleeding
Disease Location https://www.slideshare.net/mallappashalavadi/inflamm atory-bowel-disease-44916998
Pattern of Inflammation https://www.slideshare.net/mallappashalavadi/inflammatory-bowel- disease-44916998
Ulcerative Colitis Clinical Endosc 2016 49(4): 370-375
Crohns Disease Clinical Endosc 2016 49(4): 370-375
Inflammatory Bowel Disease Epidemiology Prevalence Roughly 1 in 500 Americans (201/100,000 for CD, 238/100,000 for UC) >1.4 million Americans Incidence 2-15 cases/100,000 person-years IBD is on the rise Between 2000 and 2011 in US 34% increase in UC 41% increase in CD Recent systematic review including studies 1990-2016 Incidence stable or decreasing in US Significant rising incidence in newly industrialized countries Brazil with 11% and 15% annual rise in incidence in CD and UC https://www.cdc.gov/ibd/ibd- epidemiology.htm Lancet 2018 390(10114):2769
EXTRAINTESTINAL MANIFESTATIONS OF IBD Inflammatory Bowel Dis; R. Cohen. pp258
Extraintestinal Manifestations (EIMs) Inflammatory pathology outside the gut dependent upon immune response from the intestine or shared environmental and genetic risk Up to 50% of patients with inflammatory bowel disease suffer from EIMs Risk factors for development of EIMs Duration of inflammatory bowel disease Early onset Family history Other EIMs Crohn s disease (CD)>ulcerative colitis (UC) especially colonic CD Journal of Crohn's and Colitis (2016): 239- 254
Pathogenesis of Extraintestinal Manifestations Causes of EIMs poorly understood Cross reaction of immune cells against intestinal or bacterial antigens at non-intestinal sites? Systemic inflammation induced by microbiome antigens? Genetics: EIM concordance in 70% of parent-child pairs and 84% of sibling pairs Gastroenterology 2021 Oct 161(4): 1118- 1132
Why do EIMs matter? Detrimentally affect quality of life Add to morbidity and rarely mortality associated with IBD Can support a diagnosis of inflammatory bowel disease EIMs can precede intestinal symptoms in about 25% EIM symptoms can suggest oncoming flare Deciding on IBD treatment Vedolizumab (gut-selective) versus infliximab (systemic) Identification can help direct appropriate and prompt treatment in collaboration with other specialist and primary care Rogler, G. Gastroenterology 2021 Oct 161(4): 1118-1132
IBD Patient with New Extraintestinal Symptoms Extraintestinal manifestations should be considered in a differential diagnosis Patient will often present to primary care first EIMs involve the joints, skin, and eyes most commonly Other causes of extraintestinal symptoms Unrelated conditions Comorbid immune mediated inflammatory disorders or autoimmune disease Extraintestinal complications Direct or indirect sequela of bowel inflammation or damage (e.g. vitamin deficiency) Effects of medications Drug induced lupus with biologic therapy Psoriasiform reaction to anti-TNF therapy Multiple side effects of chronic corticosteroids Opportunisitic infections Lymphoma or skin cancer
Arthritis Most common site of EIMs Reported in up to 46% of patients if pain without swelling included Incidence decreases with age Slightly more common in Crohn s disease Categorized as spondyloarthritis Others include psoriatic arthritis, ankylosing spondylitis, reactive arthritis Axial and peripheral skeletal involvement Synovitis, enthesitis, sacroiliitis, dactylitis, spondylitis, and rarely erosive arthritis can be seen Seronegative arthritis Positive RF and anti-citrullinated peptide antibodies seems to be more common than general population (10-15% vs. 5%) Journal of Crohn's and Colitis (2016): 239-254
Peripheral arthritis Peripheral arthritis Type I (oligoarticular) Affecting </= 5 joints Asymmetric and most common in ankle, knee, hips, wrist, elbow, shoulders Tracks with gut inflammation Resolves within 10 weeks or less Type II (polyarticular) Affecting >5 joints, symmetric inflammation Often affects the upper extremities (hands) Independent of gut inflammation Can last for months to years Type II may be a progression of type I over time Journal of Crohn's and Colitis (2016): 239-254
Peripheral Arthritis Diagnosis Typically clinical dx with objective signs of inflammation MRI and US will show sings of inflammation US may help in detection of enthesitis which is often missed on exam Treatment Cautious use of NSAIDs, ideally COX-2 selective, for 2 weeks or less Corticosteroids (systemic and injection) Sulfasalazine Methotrexate Anti-TNF alpha therapy (not etanercept) Leflunomide Ustekinumab Colectomy in ulcerative colitis Gastroenterology 2021 Oct 161(4): 1118- 1132 AP+T 2004, Oct 20(s4): 36-42
Axial Arthritis Associated with HLA-B27 positivity 50-70% versus >90% in AS Sacroiliitis Inflammation of the sacroiliiac joint, typically bilateral Low back or buttock pain / stiffness Common Seen in 20-50% of IBD patients on MRI Clinically significant in 8% MRI more sensitive than AP pelvic XR Ankylosing spondylitis Inflammation of the spine Can cause stiffness, pain, limited mobility If progressive can fuse the vertebra of the spine Less common Seen in 1-10% of patients Unrelated to bowel inflammation Journal of Crohn's and Colitis (2016): 239-254
Axial Arthritis Treatment Referral to Rheumatologist recommended Risk for progressive damage to the spine Physical therapy, short-term, low dose NSAIDs (COX-2 selective) Anti-TNF alpha therapy ?Tofacitinib Journal of Crohn's and Colitis (2016): 239-254
Erythema Nodosum Presentation Painful red or violet nodules 1- 5cm in diameter Typically found on the front of the legs, below the knee Seen in 4-7.5% of patients No permanent scarring, bruising can be seen as lesions heal Often tracks with bowel inflammation Treatment Leg elevation, rest, compression stockings Management of associated bowel inflammation Potassium iodide, NSAIDs Prednisone, azathioprine, and anti-TNF alpha agents Journal of Crohn's and Colitis (2016): 239-254
Pyoderma Gangrenosum Pyoderma gangrenosum Skin pustule which can become a burrowing ulcer 1 to 8+in, with purple border. Most common on the legs and around stomas Often arises at sites of trauma (pathergy); avoid biopsies Slightly more common in UC (3% vs. 2.4%) Does not track with bowel inflammation 50% of patients with PG will have inflammatory bowel disease Can lead to scarring, infection, and exposure of muscle and tendons Treatment: URGENT Wound care /ostomy nurse, dermatologist, surgeon Avoidance of ongoing trauma to the area Topical or systemic corticosteroids Anti-TNF alpha therapy Cyclosporine or tacrolimus Ostomy revision Journal of Crohn's and Colitis (2016): 239-254
Sweets Syndrome Acute febrile neutrophilic dermatosis Tender nodules or papulosquamous exanthema of arms, legs, trunk, hands, or face 80% in females Associated with malignancy, infection, azathioprine use Parallels disease activity in the gut and often associated with leukocytosis Treatment: Corticosteroids, immunomodulators, treat intestinal inflammation Gastroenterology 2021 Oct 161(4): 1118- 1132
Metastatic Crohns Disease Granulomatous inflammation of the skin Can involve any site Often seen in perineum / genitals Does not track with intestinal inflammation Treatment includes corticosteroids, anti-TNF alpha, immunomodulators Gastroenterology 2021 Oct 161(4): 1118- 1132
Oral EIMs Oral lesions Seen in 20-50% of patients with CD Seen in 8% of patients with UC More prevalent in children Aphthous stomatitis Seen on labial or buccal mucosa Often parallel bowel inflammation Associated with perianal disease Journal of Crohn's and Colitis (2016): 239-254
Oral EIMs Direct oral inflammation in Crohn s disease Cobblestone appearance to the oral mucosa Deep ulcers Periodonitis Chronic swelling and bleeding of gums leading to loss of anchoring bone and soft tissue with tooth loss Gingivitis Fissures Orofacial granulomatosis (Melkersson-Rosenthal syndrome) Chronic diffuse swelling of lower lips or face, oral ulcers, hyperplastic gingivitis, mucosal tags More common in males age 14-40 Gastroenterology 2021 Oct 161(4): 1118- 1132
Oral EIMs Treatment Annual dental visits Smoking cessation (periodonitis) Specific oral lesions in CD often treated with medications used for the bowel disease Additional topical therapy can be added to improve inflammation, pain, Topical corticosteroids Anesthetics Antiseptic mouthwash Multidisciplinary care with an ENT and dentist may be needed Journal of Crohn's and Colitis (2016): 239-254
Ocular EIMs Several parts of the eye can become inflamed in association with inflammatory bowel disease Seen in 4-12% of IBD patients Symptoms can range from asymptomatic or mild irritation to severe pain and blindness Routine eye exams recommended Journal of Crohn's and Colitis (2016): 239-254
Episcleritis Inflammation of the the outer layer of the eye Symptoms: Red conjunctiva, mild pain / grittiness , no vision changes Tracks with bowel inflammation Treatment Management of underlying bowel inflammation Corticosteroid drops, NSAIDs, systemic steroids Journal of Crohn's and Colitis (2016): 239-254
Uveitis Inflammation of the middle eye (iris, ciliary body, choroid) Bilateral eye pain, blurred vision, headache, and worsening pain with light More common in CD than UC Often independent of bowel inflammation Treatment: URGENT Anti-TNF alpha therapy, azathioprine, methotrexate Rare forms of eye inflammation Retinal vasculitis, papillitis, scleritis, scleromalacia perforans, optic neuritis. Any rapid change in vision should prompt urgent referral to an ophthalmologist Journal of Crohn's and Colitis (2016): 239-254
Hepatic EIMs Primary sclerosing cholangitis Chronic scarring of the bile ducts Symptoms; itching, malaise, fevers, abdominal pain in right upper quadrant Seen in 4-5% of those with inflammatory bowel disease UC>CD 70-80% of patients with PSC have IBD If elevated alk phos or GGT, evaluate with MRCP No effective medical therapy Disease complications Liver failure / cirrhosis, cholangitis, liver and bile duct cancer, colon cancer (10x increased risk) 12-20 year survival without liver transplant Journal of Crohn's and Colitis (2016): 239-254
Other Digestive EIMs Autoimmune hepatitis, IgG4 related cholangitis, and granulomatous hepatitis as other rare causes of liver disease Gallstone complications 2x more common in CD No association with UC Idiopathic acute pancreatitis and autoimmune pancreatitis type 2 Rare with acute pancreatitis more common in CD ?Duodenal inflammation Lipase elevation may be seen in 7% of UC patients and 9% of CD Linked to extensive colitis Medications for IBD as alternative causes of pancreatitis Gastroenterology 2021 Oct 161(4): 1118- 1132
Miscellaneous EIMs Pulmonary Rare Inflammation described involving all segments of the bronchopulmonary tree Interstitial lung disease linked with UC and granulomatous lung disease with CD Others Glomerulonephritis Pericarditis and myocarditis Amyloidosis Thromboembolism Gastroenterology 2021 Oct 161(4): 1118- 1132
Extraintestinal Manifestations Follows Gut Inflammation Erythema nodosum Pyoderma gangrenosum (50%) Type I (peripheral) arthropathy Episcleritis / Scleritis Independent of Gut Inflammation Ankylosing spondylitis Sacroiliitis Type II (axial) arthropathy Uveitis
Kidney Stones Kidney stones Calcium oxalate and uric acid stones more common, particularly with CD Impaired calcium absorption due to fat in stool More oxalate absorbed with gut barrier damage Acidosis and concentrated urine due to diarrhea Affects 10% of CD patients 4-7 years after diagnosis Particularly with multiple or long ileal resection or small bowel disease Prevention and treatment Control of diarrhea, adequate hydration, dietary calcium Medical treatments for specific stone types Surgical treatments for complicated stones Journal of Crohn's and Colitis (2016): 239-254
IBD and Venous Thromboembolism (VTE) The overall risk of VTE is 2-3x higher than the general population 60-80% of VTE occur during times of mod-severely active disease Risk during flare is 4.5 higher than remission AGA recommends VTE prophylaxis in outpatients with prior VTE during mod-severe flares Those with clots occurring exclusively after surgery excluded Once daily LMWH recommended Therapeutic anticoagulation recommended for first episode VTE if it occurs during remission Risk of recurrence is 33% at 5 years 3 mo of therapy is recommended if isolated distal DVT Nguyen G Gastroenterology (2014) 146(3):835-848
Mood Disorders 65% lifetime prevalence of mood disorder in IBD compared to 42% in community sample with other chronic disease 12 mo depression prevalence of 12-14% in IBD ~3x higher than Canadian population Higher levels of depression/anxiety in IBD than colon cancer Similar to previously reported rates for RA or DM Less than IBS patients 17% with MDD/IBD considered suicide in the last year Graff L Inflamm Bowel Dis (2009) 15(7) 1105-1118
Gut-Brain Axis Clin Therapeutics (2015): 37(5) 984-995
Mood in IBD Management Higher depression scores have been associated with higher CDAI scores Depression level at baseline correlates with total number of relapses Median time to relapse was shorter in those with depression (97 days vs. 362 days) Major depression and higher anxiety symptoms less likely to achieve remission with infliximab Mardini HE (2004) 49:492-497 Persoons P (2005) Aliment Pharmacol Ther. (2005) 22:101-110 Mittermaier C (2004) Psychosom Med 66:79-84
Managing Psychiatric Comorbidities Most vulnerable times Disease onset, disease diagnosis, and during flares Screen for mood disorders PHQ-2, PHQ-9, GAD-7 Anti-depressant therapy No high quality prospective studies, most data on paroxetine or bupropion Consider psychological treatment CBT with most support Graff L Inflamm Bowel Dis (2009) 15(7) 1105-1118














")