Immunocompromised Host Infections
An overview of immunocompromised hosts, including common defects, causes, and characteristics, with a focus on identifying and managing infections in such individuals.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Infection in the Infection in the immunocompromised immunocompromised host host Module 402
Learning objectives Learning objectives By the end of this session, you will be able to . Give a definition of an immunocompromised host. Describe common important defects and how they arise. Identify an immunocompromised patient. Explain which infections these patients predisposed to. BSAC LO 1.8 Present and recognise the characteristics of a susceptible host.
Definition of an immunocompromised host Definition of an immunocompromised host An individual who has one or more defects in the normal host defences leaving them susceptible to infection
Who is immunocompromised? Who is immunocompromised? Congenital or primary defects, which are relatively uncommon Acquired or secondary - broad category which is more common Immunosuppressive therapy related to cytotoxics, radiation, long term steroids, monoclonal therapies Physiological immunosuppression (Diabetes, elderly, pregnancy, neonates) Autoimmune disease (SLE, RA) Splenectomy (trauma, or functional asplenia) Toxicity due to alcohol Acquired immunodeficiency secondary to infection (HIV)
Immunosuppression: number or function may be affected Immunosuppression: number or function may be affected Phagocytic capacity e.g. neutropaenia or a defect in neutrophil function Cellular - T cells Humoral - B cells/immunoglobulins Complement deficiency Locally reduced immune function e.g. lymphoedema
How to spot an immunodeficient patient How to spot an immunodeficient patient History of recurrent infections or failure to thrive End organ damage eg bronchiectasis Family history Ask about alcohol, IVDU history History of immunosuppressive therapy for CTD, transplant, tumours, leukemia's, myeloma Often present with unusual or opportunistic pathogens Increased risk of severe infections
Case 1 Case 1 24 yro woman develops fever and rigors 2 days following bone marrow transplant. O/E Temp 39, pulse 100, BP 90/65 Hickman line in situ Bloods Hb 9.6, WCC 1.1 Neut <0.5, Pl 120, biochem normal, blood cultures taken
What other questions would you like to ask? What other questions would you like to ask? Functional enquiry focusing on resp, urinary, sweats etc Is the patient sick? Which other sites would you examine..mouth, ? Pus from line or erythema, skin ? Fungal infections, respiratory Any other investigations CXR, urine mcs .blood cultures from line and periphery
Neutropaenia Neutropaenia Common after chemotherapy Patients ring up with history of rigors, and if neutropaenic will be admitted to haem or onc wards. Definition of neutropaenia <0.5-1.0 x 109/l Greatest risk of infection with Neut count of <0.1 and prolonged duration
Bacterial infections predominate early in neutropaenia Fungal infections if neutropaenia is prolonged Sites of infection commonly due to lines or mucositis (mouth, gut) Important to carefully examine patient fully for source
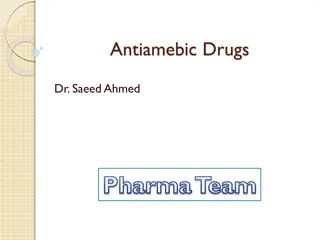
Case 1 cont. Started on empirical antibiotics intravenously and made marked improvement in 48 hours. Blood cultures isolated E.coli. Fever settles initially but recurred again after 10 days. Again no obvious physical signs and not unduly unwell. Investigation revealed neutropaenia and chest imaging showed the following after 7 days.
Aspergillus Aspergillus
Common bacterial pathogens in neutropaenics Common bacterial pathogens in neutropaenics May be Gram negative or Gram positive Line related e.g. Staph aureus, coagulase negative staphs, or environmental organisms like pseudomonas Organisms which may translocate across inflamed mucosa e.g. E.coli, Enterococci spp.
Fungal infections associated with increased Fungal infections associated with increased morbidity and mortality morbidity and mortality Candida or yeasts - often line related - may be cultured from blood Aspergillus or molds - after prolonged neutropaenia may present with fungal balls in lungs - Difficult to diagnose, may require bronchoscopy Treatment for both are antifungals (eg Fluconazole or Amphotericin) and removal of lines. Can consider using Granulocyte Colony Stimulating Factor (G-CSF) to improve neutrophil numbers
Case 2 Case 2 20 yro male involved in a motorbike road traffic accident, multiple trauma including laceration to the spleen. Due to massive blood loss required an emergency laparotomy and splenectomy. What measures should be taken to prevent subsequent infections? What organisms is he likely to be predisposed to?
Splenectomy Splenectomy May occur in traumatic situation or as a result of elective surgery Some conditions are said to result in functional asplenia eg UC, coeliac, sickle cell, SLE, RA Patients are at higher risk of developing infections due to encapsulated bacteria eg Streptococcus pneumoniae, N. meningitidis and Haemophilus influenzae
Prevention of post Prevention of post- -splenectomy infection splenectomy infection Immunization (prior to surgery if possible) Pneumovax Haemophilus influenzae B (Hib)/meningitis C (Menitorix) Meningitis B Meningitis ACWY (one month later) Influenza vaccine annually Life-long Penicillin prophylaxis if high risk Low risk may discontinue after 2 years Early therapy (eg home supply of Amoxycillin)
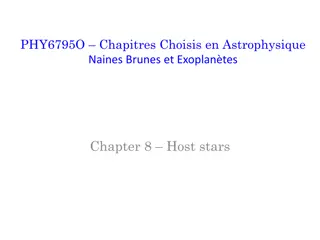
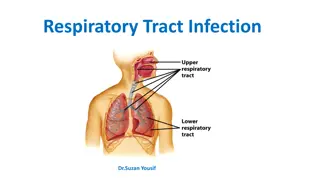
Case 3 Case 3 33 yro man presents with dry cough and breathlessness on exertion O/E pulse 100, temp 39, BP120/60, Sats 94% on RA Thin, unwell, visibly breathless Course bibasal crepitations Ix Hb 11, WC 3, Neut 2.5, lymph 0.5, Pl 50, biochem normal
Bilateral perihilar infiltrate Bilateral perihilar infiltrate
Case 3 cont. Case 3 cont. HIV test positive CD4 count 50 per mm3 Bronchoscopy findings :
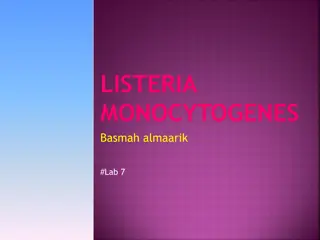
Normal alveoli and PCP Normal alveoli and PCP
Pneumocystis Pneumocystis jiroveci jiroveci causes Pneumocystis causes Pneumocystis pneumonia or PCP pneumonia or PCP Pneumocystis jiroveci stained with GMSS in BAL sample Pneumocystis jiroveci stained with IFAT seen in BAL sample Images c/o Alshahrani MY et al. doi.org/10.1016/j.sjbs.2020.04.032
Pneumocystis Pneumocystis pneumonia PCP pneumonia PCP The most common life threatening infection in AIDS patients in developed countries prior to HAART AIDS defining illness in 60% Occurs in 80% of AIDS patients in absence of antibiotic prophylaxis
PCP overview PCP overview Unicellular eukaryote-Fungus Ubiquitous geographic distribution Caused infection in patients with underlying T-lymphocyte disorders AIDS Lymphoproliferative disorders CLL Post stem cell transplantation Prolonged corticosteroid therapy
Treatment of PCP Treatment of PCP Trimethoprim/ sulfamethoxazole Dapsone/clindamycin Pentamidine iv Steroids If HIV + and CD4 count <200 should be given PCP prophylaxis + HAART
Cell mediated immunity defect Cell mediated immunity defect Aetiology AIDS Lymphoma Organ transplantation and immunosuppression Microbes Intracellular bacteria e.g. Listeria Mycobacteria Fungal e.g. cryptococcus, Pneumocystis jirovecii Viral e.g. EBV, CMV Protozoal eg Toxoplasma
Case 4 Case 4 14 yro boy, small in stature for age with recurrent sinusitis and chest infections. Had grommets as a child. How would you investigate him?
Investigations Investigations Bloods Hb 11, WC 4, Platelets 190, Biochem normal Family history CXR Lung function tests Serum immunoglobulins: IgM low, IgG low, IgA low
Hypogammaglobulinaemia Hypogammaglobulinaemia Common variable immunodeficiency (CVID) X linked agammaglobulinaemia (XLA) due to a mutation on the X chromosome affecting the btk gene coding for tyrosine kinase involved in B cell maturation Lymphomas and myeloma may also present with altered levels of immunoglobulins Commonly present with recurrent bacterial infections affecting sinuses and lungs - capsulated bugs eg. H.influenzae and pneumococci Can consider treatment with intravenous immunoglobulins
Case 5 Case 5 14 year old boy presents with a two day history of a flu like illness. His mother noticed a rash that afternoon. Had meningitis aged 3 yrs and septic arthritis aged 11. Normal developmental milestones Examination - Temp 38, Alert orientated, No neck stiffness but a non-blanching purpuric rash on trunk Hb 13.6 g/dl, WCC 22 x 109/l platelets 250 g/dl, CRP 257 Blood cultures taken Commenced on IV Ceftriaxone
Case 5 Case 5 Blood cultures grew Neisseria meningitidis He completed 7 days IV therapy Review of medical history revealed episode of Meningococcal meningitis and meningococcal septic arthritis in past ? Why recurrent episodes
Complement deficiency Complement deficiency Rare genetic disorders which results in certain components being missing Unable to form the Membrane Attack Complex (MAC) which is responsible for killing capsulated organisms such as Neisseria meningitidis
Summary Summary Neutropaenia is the most commonly observed form of immunocompromise seen in hospitals Other immunodeficiencies present with unusual opportunistic infections which do not affect a normal host You can sometimes predict the sort of infection to which a patient is most susceptible, by studying the immune defect.