Infectious diseases
Antibiotic stewardship practices, community-acquired infections, healthcare-associated infections, gram-positive and gram-negative bacteria, spirochetal diseases, viral infections, fungal and parasitic infections, surveillance and prevention of infectious diseases, common pathogens in UTI, and antibiotic-resistant bacteria are discussed in these engaging and informative 4/5th semester classes on infectious diseases.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
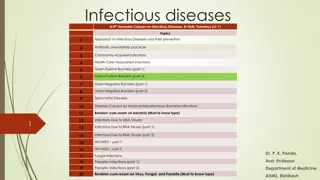
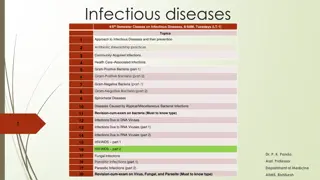
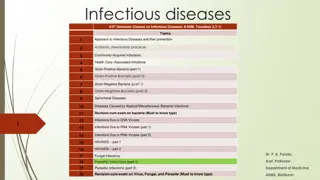
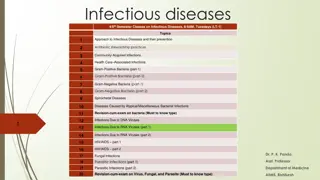
Infectious diseases 4/5thSemester Classes on Infectious Diseases, 8-9AM, Tuesdays (LT-1) Topics Approach to Infectious Diseases and their prevention 1 Antibiotic stewardship practices 2 Community-Acquired Infections 3 Health Care Associated Infections 4 Gram-Positive Bacteria (part-1) 5 Gram-Positive Bacteria (part-2) 6 Gram-Negative Bacteria (part-1) 7 Gram-Negative Bacteria (part-2) 8 Spirochetal Diseases 9 Diseases Caused by Atypical/Miscellaneous Bacterial Infections 10 Revision-cum-exam on bacteria (Must to know type) 11 Infections Due to DNA Viruses 12 1 Infections Due to RNA Viruses (part 1) 13 Infections Due to RNA Viruses (part 2) 14 HIV/AIDS part 1 15 HIV/AIDS part 2 16 Dr. P. K. Panda, 17 18 Fungal Infections Parasitic Infections (part 1) Asst. Professor Department of Medicine 19 Parasitic Infections (part 2) 20 Revision-cum-exam on Virus, Fungal, and Parasite (Must to know type) AIIMS, Rishikesh
Surveillance, prevention, and treatment Zero tolerance all health care associated infections should be avoidable with strict application of evidence-based prevention guidelines Nosocomial infections follow basic epidemiologic patterns The mode of transmission usually is either cross-infection or autoinoculation Surveillance requires review of microbiology laboratory results, shoe-leather epidemiology on nursing wards, and application of standardized definitions of infection House-wide surveillance, Not used now-a-days
UTI (3040%) GROUP A STREPTOCOCCAL INFECTIONS SURGICAL WOUND INFECTIONS (15 20%) FUNGAL INFECTIONS PNEUMONIA (10 15%) LEGIONELLOSIS INFECTIONS RELATED TO VASCULAR ACCESS (10 15%) ANTIBIOTIC-RESISTANT BACTERIA CA-MRSA VIRAL RESPIRATORY INFECTIONS Plasmid mediated resistance to fluoroquinolones NOSOCOMIAL DIARRHEA Metallo- -lactamase mediated resistance to carbapenems KPCs (carbapenemase-producing strains of K. pneumonia) CHICKENPOX Panresistant strains of Acinetobacter TUBERCULOSIS
UTI The most common pathogens are Escherichia coli, nosocomial gram-negative bacilli, enterococci, and Candida Patients with chronic indwelling bladder catheters, especially those in long- term-care facilities, catheter flora may differ from actual urinary tract pathogens. Therefore, obtain a freshly voided urine specimen Repeat the culture to verify the persistence of infection after treatment initiation Other source of infection in a febrile hospitalized patient should be evaluated e.g. recovery of Staphylococcus aureus from urine cultures may result from hematogenous seeding Candida is now the most common pathogen in intensive care units (ICUs)associated UTI, treatment is recommended only when there is; upper-pole or bladder-wall invasion, obstruction, neutropenia, or immunosuppression
SURGICAL WOUND INFECTIONS The most common pathogens are S. aureus, coagulase-negative staphylococci, and enteric and anaerobic bacteria. In rapidly progressing postoperative infections manifesting within 24 48 h of a surgical procedure, group A streptococcal or clostridial infection more common
PNEUMONIA Early-onset nosocomial pneumonia, which manifests within the first 4 days of hospitalization, is most often caused by community-acquired pathogens such as Streptococcus pneumonia and Haemophilus species Late-onset pneumonias most commonly are due to S. aureus, P. aeruginosa, Enterobacter species, Klebsiella pneumoniae, or Acinetobacter
INFECTIONS RELATED TO VASCULAR ACCESS The most common pathogens include coagulase-negative staphylococci, S. aureus, enterococci, nosocomial gram-negative bacilli, and Candida
Standard precautions are designed for the care of all patients in hospitals and aim to reduce the risk of transmission of microorganisms from both recognized and unrecognized sources These precautions include gloving as well as hand cleansing for potential contact with (1) blood; (2) all other body fluids, secretions, and excretions, whether or not they contain visible blood; (3) nonintact skin; and (4) mucous Membranes. Depending on exposure risks, standard precautions also include use of N95 respirators, surgical face masks, or glove and gown for airborne, droplet, or contact exposure respectively Other measures of standard precautions; Prevention of needle stick injury Environmental cleansing and spill management Waste management
EMPLOYEE HEALTH SERVICE Contagious-disease history can be taken; Evidence of immunity to a variety of diseases, such as hepatitis B, chickenpox, measles, mumps, and rubella, can be sought; Immunizations for hepatitis B, measles, mumps, rubella, varicella, Influenza, and pertussis can be given as needed; Baseline tuberculosis testing can be performed; Education about personal responsibility for infection control can be initiated
Protocols for dealing with workers exposed to contagious diseases (e.g., influenza) and those percutaneously or mucosally exposed to the blood of patients infected with HIV or hepatitis B or C virus. For example, postexposure HIV prophylaxis (PEP) Protocols for dealing with caregivers who have common contagious diseases (such as chickenpox, group A streptococcal infection, influenza or another respiratory infection, or infectious diarrhea) and for those who have less common but high-visibility public health problems (such as chronic hepatitis B or C or HIV infection)


")