Insights on Neuroimaging: Annual Meeting Highlights
Comprehensive overview of the American Society of Neuroimaging annual meeting covering topics like MRI safety, equipment costs, operational insights, revenue projections, and scaling strategies.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
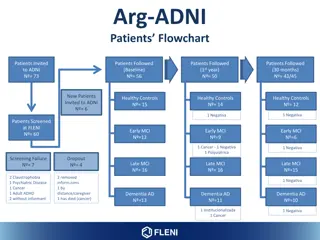
American Society of Neuroimaging Annual Meeting Friday, January 15, 2016, 3-4pm Joseph V. Fritz, PhD, CEO, Dent Neurologic Institute, Amherst, NY, 14226 Vernon Rowe, M.D. CEO, Rowe Neurology Institute, Lenexa, KS 66214
Scanner Room Equipment Room Tech Area Outside Equipment Fringe Fields Power Vibration Security
Forces on magnetic materials (increases with B0) Type of implanted device (See www.MRISafety.com) 5G safety line (10,000 G = 1 T) Dizziness (B0 at fringe) Heating/Electrical Conduction (B1 field = RF Pulses) SAR of 1 W/kg increases temp 1 degC/hour Normal mode <2, Medical Supervision <4, IRB if >4 Nerve Stimulation (Gradient switching, dB/dt < 20 T/s) EPI, other fast sequences Induced currents in Tatoos, wire leads Acoustic Noise < 85dB without hearing protection Nephrogenic Systemic Fibrosis (NSF) Avoid Contrast if GFR < 30 Greater reported incidence for Omniscan, Magnevist and Optimark
Low Field Open New 1T Open $400,000 $1.5M --------------------- $600,000 $1.2M --------------------- $900,000 $1.9M --------------------- $6M, plus $1M siting Refurb 1.5T New 1.5T Refurb 3T New 3T 7T
Equipment (MRI, PACS, etc) eg$1.5M operating lease Service New Installation eg$400,000 5yr capital lease Rent eg$20/sfx 1200sf Staff egRT@$25, clerical@$15 Legal, Management, Physicist $21,000 $12,000 $ 7,500 $ 2,000 $10,000 $ 1,000 $53,000 $200 270 scans per month= 14 scans per day Technical Margin per scan Breakeven (Costs/margin)
Operate 40hrs/week, hrper patient 320 scans per month = 50 scans beyond breakeven TC profit = $200 x 50 = $ 10,000 monthly $120,000 annually Annual PC Revenue = $60/scan x 320 x 12 (< 80 hrs/mo) = $200K New 1.5T Scanner Justification? Need about 10-15/day x 5d/week 1 scan per day beyond b.e. = $60 -$100K annual profit New Neuro Patient 50% need MRI 20-30 new pat/d >4 MDs with PA support for f/u Scale Down the Scanner Technology for Smaller Practices
Can you assume 1 MRI per 2 Consults? eg 10 MRI per day = 20 consults/day Depends on subspecialty mix, cost of equipment, local financials Assumes referring physician relies on neurologist to order Long wait for neurology consult will result in more outside imaging Rapid Access to Physician Consults Critical Use Advanced Practice Providers (PA, NP) to free up MD consults Minimum # MDs depends on ability to shift followups to APP; e.g. 4 MDs at 5 consults per day each
Fee schedules reducing Obstacles and costs for authorization Reader credentialing with Payers Payer contract and utilization monitoring when self-referring Missing non-neuro pathology Local Politics
Pre-Stark Post-Stark and the IOASE Importance of the IOASE to other specialties of medicine as well as to Neuroimaging Hutchinson et al. refuting GAO report
Coalition for Patient Centered Imaging Other outpatient imaging and treatment specialties Intense lobbying of House and Senate to preserve IOASE, successful Data from the Milliman study finally in IOASE saves money
Hospital-centered healthcare vs independent physician- centered healthcare CMS has rewarded hospital-based care with facility fees and higher payment premiums over physician-centered care Alternative payment models like ACO s, most hospital- centered, fostered by the ACA haven t worked in cost reduction EMR s, even from a single vendor, don t talk to each other by design. Most recent budget deal ends hospital preferential payment for newly acquired off-campus practices after 2017 Insurance consolidation, increasing premiums and deductibles, are merely a reaction to hospital consolidation and market clout
As cost and quality transparency become the watchwords, hospital-centered healthcare will not be able to compete with physician-centered healthcare
Marilyn Tavener and Andrew Slavitt The Big Question: Hospital-employed or independent practice
Dual agency problem inherent in hospital employment Hospitals not likely to bend from Radiology Contracts to incorporate Neurologist Neuroimagers rare exceptions lawsuit experience of CIN more typical
Can we financially survive until the pendulum swings the other way?
How about optimal health care for the half of the country that lives in rural or urban cluster environments? Case study
Financials of MRI Equipment MRI and X-Ray Office Magnet Web-based PACS for image storage and retrieval Images are portable but must be interpreted according to state law Web-based EMR Athena for revenue cycle management and patient record retrieval
Accredited sleep disorders center Headache Center MS Center Memory Loss Center Clinical Trials incorporation into the PA Neurophysiology EMG, EEG, Long term monitoring Infusion Center Physical Therapy
Importance of web presence to make potential patients aware and give them a choice Potential for RNI to serve as a model for an Independent Neurology Practice in rural and urban cluster environments, as well as urban and urban area environments Incorporation of Neurosurgery, outpatient Radiation Oncology, PT, Pain Management, Neuro-oncology, others, in larger groups possible to insure survival of NI by Neurologists Doctor-owned hospitals CIN experience
Critical for a Future Role for Neuroimaging in Neurology Practice Local--with insurance companies State legislature with educators (lobbyists) and friendly legislators KIP, Inc. to sponsor compulsory facility fee notification by hospitals when KMS declined to support National Professional Organizations AMA, AAN, ASN US Congress Doctors caucus in the House, and Doctors in the Senate question hospital not- for-profit status New Jersey case Kansas true charity care vs bad debt Enemies of Neurologists doing NI are relentless we have to be relentless too: NI critical to patient care No one will rescue us: we have to rescue ourselves David and Goliath David always wins per Malcom Gladwell
Independent Neurologists can survive and even thrive in the current healthcare environment Crucial to that survival is control of and access to outpatient Advanced Imaging Advocacy at all levels crucial to that survival, as the pendulum swings
Fritz, J. The practice of neuroimaging within a neurology office setting, Neurology in Clinical Practice, December 2013 vol. 3 no. 6 501-509 Hutchinson M, Rowe E, Kushner M, Rowe, V. Appropriate use of advanced imaging services by providers who self-refer is saving Medicare Billions, Journal of Neuroimaging, Volume 23, Issue 1, pages 159 161, January 2013




")

")