Intensive Home Support Service (IHSS) - Urgent Community Response
The Intensive Home Support Service (IHSS) provides 2-hour urgent community response and hospital-at-home care for individuals facing acute health crises. Led by Consultant Practitioner Matthew Morrissey, the service offers clinical assessments, interventions, and access to specialist care teams for conditions such as COPD exacerbation, heart failure, and more. Operating 24/7, IHSS aims to prevent unnecessary hospital admissions and provide comprehensive care in the comfort of patients' homes.

Uploaded on Mar 10, 2025 | 0 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Intensive Home Support Service (IHSS) 2-Hour Urgent Community Response & Hospital at Home Provider Matthew Morrissey Consultant Practitioner
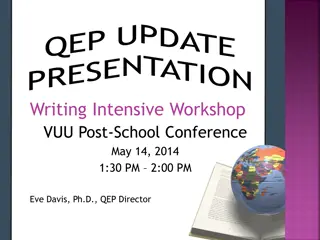
Typical Presentations Referral Process and Opening Times Acute deterioration in functional ability at risk of hospital admission Exacerbation of long-term condition, at risk of hospital admission Acute social care/carer crisis Falls due to non-medical (extrinsic) cause without apparent injury Clinical conditions may include: If your patient needs an Urgent Community Response (UCR) / Hospital at Home assessment and is aged 18 or over, then please contact the community services single point of access via Intermediate Care Allocation Team (ICAT) on : 01282 805989 Acute exacerbation of COPD/LRTI Suspected decompensated Heart Failure Urinary Tract Infection Delirium/Acute Confusion Acute diarrhoea/vomiting Monitoring of electrolyte abnormalities Acute Skin Infection Response times are based on clinical need and can be within 2 hours from point of referral to ICAT Visits are available 24 hours/day over any 7 day period INTENSIVE HOME SUPPORT SERVICE : 01282 805989 Interventions: Exclusions: The service will assess patients individual health needs to identify the care they require. This will involve a full holistic assessment, providing any necessary equipment and agreeing a plan of care with the patient. Hospital conveyance/admission is in the persons best interests Acute Mental health crisis as the primary presentation Acute exacerbation of Asthma Minor ailments Acute Surgical Presentations Singular clinical tasks e.g. bloods alone without need for holistic management As part of this, interventions may include: Advanced assessment, clinical examination, diagnosis & non-medical prescribing. Obtaining blood for laboratory analysis Monitoring, including blood pressure and temperature, ECG Support, information and education Therapy assessment and equipment Mental health management Daily MDT with access to a GP and Hospital Doctor Commission crisis care packages via ICAT
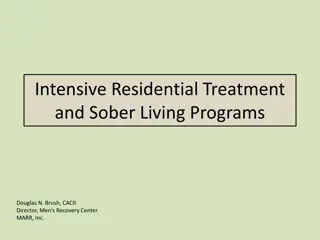
IHSS Hospital at Home/Virtual Ward DIRECT CLINICAL PHONE: 01282 805729 Consultant Practitioner led service to manage greater clinical complexity MDT including input from Respiratory Medicine, Primary Care, Specialist Palliative Care and Therapy Access to diagnostics e.g. ECG, XR, Ultrasound, CT Scan Remote/digital monitoring via wearable technology Advanced Care Planning -IV Fluid Bolus (Phase 1) Pilot March/April 2024 embedded as business as usual -IV Fluid Maintenance (Phase 2) Pilot ?November 2024 Developing interventional pathways -IV Furosemide -Acute oxygen therapy (Community Acquired Pneumonia step-down) -Continuous monitoring pilot (Vitalerter) HR, RR, Sp02, Falls Detection July 2024 -Early stages of discussing mobile x-ray at home
Operational Model Supported by SPA Service which combines Health & Social care provision (Crisis Care/Social Work assessment) Referral Sources: Self (known patients) Small ED Front Door team pulling patients out Mon- Fri 160 Virtual Beds Occupancy between 65-80% 24-hour service for past 2 years GP NWAS Secondary Care Care Homes Other Trusted Assessors (e.g. Social Workers, Carers, Speciality Teams)
Staffing Model (Combined UCR & VW Funded) 4 Consultant Practitioners ED, Critical Care Outreach/Acute Care and Community background 1 x Respiratory Consultant 2 PA s 1 x GP Medical Lead 6 PA s 2 x GP 4 PA total 2 x ST5 Frailty Doctors, 2 GPST trainees 7 x Advanced Clinical Practitioner, 1 x Trainee (Jan 2025) 17 x Band 7 Senior Community Practitioners 28 x Band 6 Community Practitioners 10 x Therapy Practitioners (OT/PT Band 7-5) 13 x Band 4 Assistant Practitioners / Nurse Associates 1 x Mental Health Practitioner (NMP Band 7)
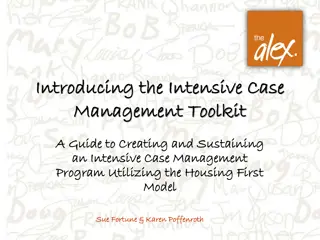
Recent Investigations Background Recent ECHO pre chemotherapy Breast cancer T2 N2 M0 on chemotherapy and radiotherapy Case Study 1 Preserved ejection fraction 60-65% COPD on SBOT Magnesium 0.43 Hypertension Potassium 2.8 Previous pleural effusion 62 y/o female Self-referral due to breathlessness. On antibiotics for suspected cellulitis to leg. Bloods completed by chemo unit which highlighted hypomagnesium and hypokalaemia. Significant new lower limb swelling. Initially visited as 2 hour UCR then escalated to Hospital at Home caseload for assessment and ongoing management. Clinical Narrative Multiple problems but main concern was lower limb swelling impacting mobility and skin at risk. Treated as cellulitis by chemotherapy unit but no evidence of infection. Breathlessness had developed and chest was quiet to left base - commenced on diuretics toreduce oedema and treated as HFpEF 40mg Furosemide BD for 7 days. Urgent outpatient chest xray completed to exclude new pleural effusion showed opacification which may represent infection (no infective symptoms at this stage) - treated with antibiotics and symptoms improved 2.5-3 litre fluid intake daily advised to reduce to 1.5 - 2 litres. Replaced potassium and magnesium orally resolved following treatment Developed pain and erythema around PICC line site cultures obtained peripherally and from line no growth Advance care planning and discussion around ceilings of care and treatment wanted Length of Stay 12 days




")