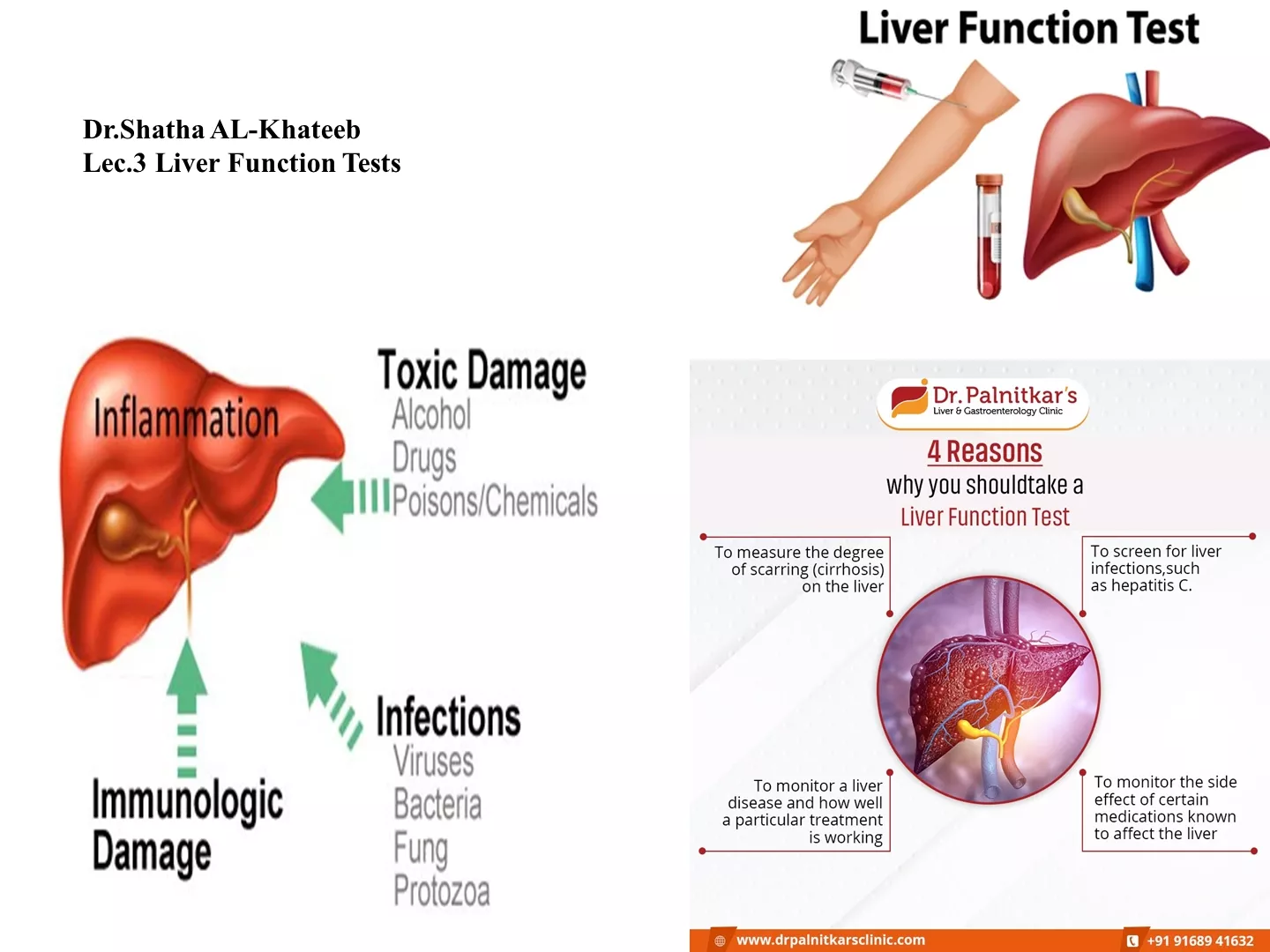
Intestinal obstruction
Intestinal obstruction can be classified into dynamic and adynamic types, each with distinct pathophysiological changes. Dynamic obstruction involves increased peristalsis in response to a mechanical blockage, leading to bowel dilatation, gas accumulation, and fluid retention. Clinical features vary based on the site and completeness of the obstruction. Learn more about its classifications and manifestations in this detailed guide.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
CLASSIFICATION Intestinal obstruction may be classified into two types: Dynamic, peristalsis is working against a mechanical obstruction. It may occur in an acute or a chronic form. Adynamic, in which there is no mechanical obstruction; peristalsis is absent or inadequate (e.g. paralytic ileus or pseudo-obstruction).
PATHOPHYSIOLOGY In dynamic (mechanical) obstruction, the bowel proximal to the obstruction dilates and the bowel below the obstruction exhibits normal peristalsis and absorption until it becomes empty and collapses. Initially, proximal peristalsis is increased in an attempt to overcome the obstruction. If the obstruction is not relieved, the bowel continues to dilate; ultimately there is a reduction in peristaltic strength, resulting in flaccidity and paralysis. The distension proximal to an obstruction is caused by two factors: Gas: there is a significant overgrowth of both aerobic and anaerobic organisms, resulting in considerable gas production. Fluid: this is made up of the various digestive juices. (saliva 500mL, bile 500mL, pancreatic secretions 500mL, gastric secretions 1 litre all per 24 hours). This accumulates in the gut lumen as absorption by the obstructed gut is retarded.
Obstruction by adhesions and bands The common causes of intra-abdominal adhesions:
CLINICAL FEATURES OF INTESTINAL OBSTRUCTION classified clinically into two types: small bowel obstruction high or low; large bowel obstruction. The nature of the presentation will also be influenced by whether the obstruction is: complete; incomplete.
ADYNAMIC OBSTRUCTION Paralytic ileus is failure of transmission of peristaltic waves secondary to neuromuscular failure (i.e. in the myenteric and submucous plexuses). The resultant stasis leads to accumulation of fluid and gas within the bowel, associated distension, vomiting, absence of bowel sounds and absolute constipation. Varieties Postoperative: occurs after any abdominal procedure and is self-limiting, with a variable duration of 24 72 hours. Postoperative ileus may be prolonged in the presence of hypoproteinemia or metabolic abnormality. Infection: intra-abdominal sepsis >>>localized or generalized ileus. Reflex ileus: following fractures of the spine or ribs, retroperitoneal haemorrhage or even the application of a plaster jacket. Metabolic: uremia and hypokalemia