Kidney Function Tests: Clinical Insights
The main functional unit of the kidney is the nephron, responsible for urine formation through mechanisms like glomerular filtration and tubular reabsorption. Kidney function tests help diagnose kidney disorders and systemic diseases affecting kidney functioning. They include macroscopic examination involving color, odor, pH, specific gravity, and volume. Abnormal findings in these tests can indicate various diseases or conditions. Learn more about the significance of urine examination for diagnosing kidney issues.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
KIDNEY FUNCTION TESTS part- 1 Clinical Tests Lec. 4 3rd Grade Fall Semester 2021-2022 Goran N. Saleh goran.nori@tiu.edu.iq 6/12/2021
Introduction The main functional unit of kidney is nephron each kidney consists of millions o nephrons Urine is formed by the following mechanism 1.glomerularfiltration 2.tubular reabsorbtion 3.tubularsecretion
PURPOSE To diagnose the disease or disorders of kidneys and urinary tract and other systematic diseases that effect the kidney functioning Urine examinationis usually employed to diagnose most of the kidney disorders Urine examination is classified into 3 types 1.macroscopic examination 2.microscopicexamination 3.chemical examination
MACROSCOPICEXAMINATION Color Odor PH Specificgravity Volume
Color: normal color of urine is pale yellow due to urocrome Abnormal colors are observed during diseased state Various colors and corresponding diseases are as follows RED hematurea, beetroot juiceintake BLUE-cholera YELLOW-BROWN bilirubin YELLOW -GREEN biliverdin ORANGE excessivesweat,fever BLACK melanin JAUNDCE
Odor: smell of urine is usually lightpungent Various other smells are also observed AROMATIC :volatile fattyacids AMMONICAL: due to bacterialaction FRUITY ODOR : ketonurea Volume: normal value is1000- 2000/24hrs(depending upon waterintake) Increase in urine levels POLYUREA (more than 2000ml) This may be due to certain drugs,IV solutions,diabetis mellitus etc
Decrease in urine levels: (less than 400ml/24hrs) This is called OLIGUREA ANUREA : less than 100 ml of urine in 24 hrs These conditions may be due to dehydration, congestive heart failure , due to renal tract obstructionetc PH: Normal PH of urine is 6 it may be between 5-9 depending upon diet High ph : (classic renal alkalosis) due to sodium carbonate containing drugs, strictvegetarian Lower ph:(classic renal acidosis) due to ammoniumchloridecontainingdrugs,starvation,keto sis,fever,diabetis
Specific gravity: normal value of specific gravity is 1.001-1.040 Increase in specific gravity is due to dehydration, fever, vomiting, diarrhea ,congestive heart failure, diabetesmellitus Decrease in specific gravity is due todiabetes insipidus CHEMICALEXAMINATION Test for various abnormalities like : Proteins Sugars Ketones Bile salts and bile pigments Blood
PROTIENS: TEST OBSERVATION INFERENCE Sulphosalicylic acid Whiteprecipitate test: 3ml of urine + is formed sulphosalicyclic acid drop by drop Presenceof proteins Helis nitric acid ring test :3ml conc nitric acid+urine sample drop wise from sides of testtube White ring is formed at the junction oftwo layers Presenceof proteins Heatcoagulation: boil 5ml of urine sample for 5 min Turbidityis observed Presenceof proteins
Presence of protein inurine is called proteinurea Various causesare Severeexercise High proteindiet Pregnancy Kidneydisease Damage to lower urinarytract Fasting
SUGARS: TEST Benedictsreagent test : 2mlurine +2ml benedicts qualitativereagent boil for 2 min and cool OBSERVATION a)Green ppt b)Brick red ppt c)Yellowppt INFERENCE a)1%glucose b)2%glucose c) More than 2% glucose Fehling's reagent test: 2ml of Fehling's A and Fehling s B +2ml urine boil for 2 to5 minutes Red or yellow ppt is formed Presenceof Glucose Presence of glucose in urine glucosurea this may be due to diabetes mellitus ,hypertension, corticosterol drugs etc
Ketones: TEST OBSERVATION INFERENCE Ruthera s test : 5ml urine + small amt of ammonium sulphate + 2 drops of sodium nitroprusside+2ml of stong ammonia sol and wait for 10 min Permanganate colour is observed Presence of ketone bodies Presence of ketone bodies in urine is called ketonurea this may be due to starvation, excessive fatty acid metabolism, pregnancy
Bile salts: TEST OBSERVATION INFERENCE Sulphur powder test: Take 5mlurine in a beaker and sprinkle sublimed sulphur powder Presence of bile salts Powdersinks to bottom Prescence of bilesaltsinurinemaybedueto jaundice obstructiontobiliarytract liverdiseases
Bile pigments: TEST OBSERVATION INFERENCE Gemelin test :10ml of urine + 2 to 3 drops of dil HCl filter it , allow the filter paper to dry and put a drop of HNO3 Coloration ofpaper in following order Green Blue Violet Red Yellowishred Presence of bile pigments Hellis nitric acid test: 3ml of conc HNO3 + add urine drop wise slowly Presence ofbile pigments Fine ply ofcolors is observed Apart from these tests vanderbergs reaction fouchets tests are also employed
Prescence of bile salts in urine may be due to Jaundice (hemolytic or obstructive) obstruction to biliarytract liverdiseases
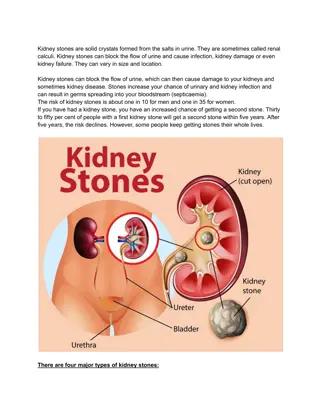
Blood: TEST Benzidine test :2ml urine + few ml of H2O2 + pinch of bezidine in acetic acid OBSERVATION INFERENCE Green colouris observed Presence of blood Presenceofbloodinurineiscalledhematurea various causes forhematureaare Renalcalculi Glomerulonephritis SevereUTI Renaltracttumor
Microscopic examination : In this the analysis is done simply by pouring the urine sample into test tube and centrifuging it for 5 min the top liquid part is discarded and the sediment left at the bottom is mixed with 1 drop of urine and is studied under a microscope Cells Crystals Casts Microorganisms Parasites etc areobserved
CELLS: Few epithelial cells and RBC are observed occasionally in urine This may be due to fever or urinary tract calculi or acute renal damage orglomerulonephritis CRYSTALS: Various crystals are found in the acidic urine like Uric acid crystals Calcium oxalate crystals Cystine crystals etc
Crystals found in basic urine are carbonate and phosphate crystals
CASTS : Urinary casts are cylindrical structures produced by the kidney and present in the urine in certain disease states. They form in the distal convoluted tubule and collecting ducts of nephrons, then dislodge and pass into the urine, where they can be detected by microscopy. These casts are of two types CELLULARCASTS RBC WBC epithelial ACELLULARCASTS Hyaline casts fattycasts waxycasts pigment casts
NPN CONSTITUENTS OF URIne : NPN stands for non protein nitrogenouscompounds The nitrogen content of substancesother than protein in blood, tissues, and wastematerials. i.e nitrogen associated with Urea uricacid creatine polypeptides. Approximately one half of the nonprotein nitrogen in the blood is associated with urea
Clinically significant NPN constituents along with approximate plasma conc are listed below Urea Aminoacids - 20% Uricacid - 20% Creatinine - 5% Creatine - 2% Ammonia - 0.2% - 45% UREA : BUN stands for blood urea nitrogen.Urea nitrogenis formed when protein breaksdown. A test can be done to measure the amount of urea nitrogen in the blood. The BUN test is often doneto check kidney function.
The normal result is generally 6 -20mg/dL. Higher-than-normal levels(Azotemia) may be due to: Congestive heartfaliure Excessive protein levels in the gastrointestinaltract Gastrointestinal bleeding Hypovolemia(dehydration) Heartattack Kidney disease, including glomerulonephritis, pyelonephritis, and acute tubularnecrosis Kidney failure(uremia) Shock Urinary tractobstruction
Lower-than-normal levels may be due to: Liver failure Low proteindiet Malnutrition Over-hydration ESTIMATION OF UREA:








 This")