Explore the epidemiology, histopathology, anatomy, and TNM classification of laryngeal cancer. Learn about the diagnosis methods and treatment options for this condition. Identify key symptoms and diagnostic tests for early detection. Images and detailed information included.
Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
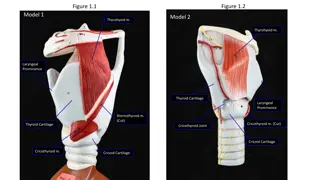
CANCER LARYNX Duong Thi My Cancer larynx, Disease of ear, nose, throat, head and neck surgery
EPIDEMIOLOGY AND HISTOPATHOLOGY AETIOLOGY ANATOMY - SUBDIVISION TNM CLASSIFICATION AND STAGING DIAGNOSIS OF LARYNGEAL CANCER TREATMENT OF LARYNGEAL CANCER I. II. III. IV. V. VI.
I. EPIDEMIOLOGY AND HISTOPATHOLOGY - 2,63% of all body cancer - M : F = 10:1 - Age group: 40-70 - 90 95% : squamous cell carcinoma II. AETIOLOGY American Cancer Society: Cancer Facts and Figures 2008. Atlanta, Ga: American Cancer Society, 2008
IV. TNM CLASSIFICATION AND STAGING Source: Greene FL, Page DL, Fleming ID, et al. (editors). American Joint Committee on Cancer Staging Manual, 6th edition, New York: Springer-Verlag, 2002
V. DIAGNOSIS OF LARYNGEAL CANCER History. any patient in cancer age group having persistent or gradually increasing hoarseness for 3 weeks must have laryngeal examination to exclude cancer - Other symptoms: Throat pain, dysphagia, referred pain in the ear, or mass of lymph nodes in the neck - Late feature: Weight loss, stridor, respiratory obstruction, halitosis 1. 2. Indirect laryngoscopy - Appearance of lesion - Vocal cord mobility - Extent of disease
V. DIAGNOSIS OF LARYNGEAL CANCER 3. Examination of neck - Extralaryngeal spread of disease - Nodal metastasis 4. Radiography: CT scan or MRI: - Evaluate pre-epiglottic or paraglottic space - Laryngeal cartilage erosion - Cervical node metastasis Certain diagnostic test 5. Direct laryngoscopy - The hidden areas of larynx - Extent of disease 6. Supravital staining and biopsy
VI. TREATMENT OF LARYNGEAL CANCER Site and extent of lesion (T) Presenceor absence of Nodes (N) Distant Metastases (M) Treatment Organ preservation Radiotherapy Surgery Combined therapy Endoscopic CO2 laser excision Total laryngectomy Conservation laryngeal surgery Surgery with pre- or postoperative radiotherapy
GLOTTIC CARCINOMA 1. Carcinoma in situ: Transoral endoscopic CO2 laser biopsy stripping of vocal cord carcinoma in situ invasive carcinoma Regular follow-up. radiotherapy
Invasive carcinoma T1 carcinoma with extension to anterior commissure carcinoma with extension to arytenoid carcinoma Radiotherapy Radiotherapy frontolateral partial laryngectomy Excision of cord total laryngectomy
- Mobility of vocal cord? - Involvement of anterior commissure and/or arytenoid? T2N0 cancer Cord mobile Cord mobility impaired or Involvement of anterior commissure or arytenoid Radiotherapy Failure Conservation laryngectomy Conservation laryngectomy Failure Failure Total laryngectomy neck dissection Total laryngectomy neck dissection
If nodes are palpable T3 total laryngectomy + neck dissection T4 combined therapy: surgery + P.R Only Palliative treatment Subglottic cancer T1,T2 T3,T4 Total laryngectomy and P.R Radiotherapy P.R: postoperative radiotherapy
Supraglottic cancer T2 T3 , T4 T1 Lung function Radiation or total laryngectomy with neck dissection and P.R to neck excised with CO2 laser good poor supraglottic laryngectomy With or without neck dissection radiotherapy
Radiotherapy - Cord mobility: normal - Invade cartilage or cervical nodes: no Total laryngectomy: - T3 lesions (i.e. with cord fixed) - All T4 lesions - Invasion of thyroid or cricoid cartilage - Bilateral arytenoid cartilage involvement - Lesions of posterior commissure - Failure after radiotherapy or conservation surgery - Transglottic cancers, i.e. tumours involving supraglottis and glottis across the ventricle, causing fixation of the vocal cord