Larynx Cancer: Causes, Types, and Symptoms
Learn about larynx cancer, including its causes, risk factors, types, benign tumors, clinical features, signs of metastasis, and diagnostic tests. Men over 60 are more susceptible to this condition, with common causes being tobacco use and voice strain. Recognizing symptoms like persistent hoarseness, difficulty swallowing, and throat lumps can aid in early detection and treatment.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Most common in people between the ages of 60 and 70 years Men is more prone to get Ca larynx than women
Causes and risk factors Other factors straining the voice Tobacco Combined effects of alcohol and tobacco Asbestos Paint fumes Wood dust Chemical Chronic laryngitis Nutritional deficiencies Family predisposition Age more than 60 Gender- males Race african americans Weakened immune system
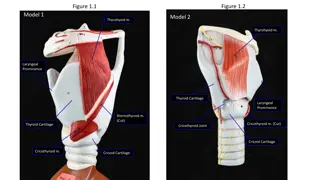
Types Squamous cell carcinoma 95% - develops in the flat, skin like squamous cells that cover the surface of the epiglottis, vocal cords and other parts of the larynx Adenocarcinoma starts in the adenomatous cells that scattered around the surface of the larynx. Adenomatous cells are gland cells that produce mucus Sarcoma starts in the connective tissues. These are the supporting tissues of the body, such as bone, muscle and nerves. Chondrosarcomas cancers in the cartilage of larynx
Benign tumours Giant cell tumors Granular cell tumours Benign tumours of muscle (rhabdomyomas) Benign tumours of nerves (schwannomas) Laryngeal nodules caused by smoking, acid reflux and straining the voice Papillomas these are wart like growth on the larynx. Caused by virus called human papilloma virus (HPV)
Clinical features Persistent hoarseness associated with otalgia and dyphagia The voice may sound harsh, raspy, and lower in pitch A smoker, who becomes progressively hoarse or is hoarse for longer than 2 weeks should be urged to seek medical attention. A lump may be felt in the neck a cough that doesn't go away persistent sore throat breathing difficulties, or feeling that something is catching in the throat ear pain, coughing up of blood
Signs of metastasis lump in the throat, pain in the adams apple that radiates to the ear, dyspnea, dysphagia, enlarged lymph nodes and cough. Lymphadenopathy, weight loss, general weakness may occur.
Diagnostic test Complete history and physical examination of head and neck Barium swallow to rule out metastasis to esophagus Biopsy for pathologic confirmation of the diagnosis Chest x ray examination to determine whether there is metastasis to lung, a second primary tumor, or chronic obstructive pulmonary disease.
Endoscopy virtual endoscopy (3 dimentional view of hollow structures is conducted through the utilization of high resolution imaging and unique computer processing methods) Computed tomography scan- to determine if there is metastasis to lymph nodes or adjacent structures Fiberoptic laryngoscopy to determine diagnosis, locate mass or ulceration. MRI, PET SCAN
Management Goals of treatment Cure of the disease Preservation of safe, effective swallowing Preservation of useful voice Avoidance of permanent Tracheostomy Treatment option includes: Surgery Radiation therapy chemotherapy
Prognosis depends on the tumor stage, the patients gender and age, and pathologic features of the tumor, including the grade and depth of infiltration Complete dental examination should be done. If any dental problem is there, it should be resolved before surgery and radiotherapy Early stage tumors and lesions without lymph node involvement, radiation therapy or surgery may effective. Chemo radiotherapy provides high rates of laryngeal preservation.
Surgical management Goals Minimizing the effects of surgery on speech, swallowing and breathing Maximizing the cure of cancer
Patient with more extensive tumors (T3 and T4) require a combined approach of surgical resection and preoperative and post operative radiotherapy Chemotherapy with cisplatin and 5-flurouracil along with radiotherapy is also suggested.
Hemilaryngectomy/ vertical partial laryngectomy In this half of the larynx is removed This procedure is usually well tolerated The patient not allowed to swallow for 7 to 10 days postoperatively Removal of more than half the larynx or a portion of the second vocal cord is called a SUBTOTAL LARYNGECTOMY.
Opening into larynx through thyroid cartilage with removal of diseased false cord, and one side thyroid cartilage Voice result hoarse voice Swallowing ability initially need swallowing therapy to learn how to swallow without aspirating
Supragloticlaryngectomy When cancer invades the supraglottis, a supraglottic laryngectomy is done True vocal cords are preserved Aspiration may occur because the major reflex arc that causes closure of the larynx is initiated by sensory receptors in the supraglottic larynx, which has been removed These patients need special swallowing training postoperatively
When aspiration is suspected the patient swallows a drink with methylene blue dye, grape juice or food coloring added then check the tracheal secretions Horizontal incision passes above true cords (leaving cords intact) with removal of epiglottis and diseased tissue Voice result normal voice Swallowing therapy should be start initially itself
After a partial laryngectomy a temporary tracheostomy tube is inserted It is removed when edema in the surrounding tissues subsides Patient is not allowed to use voice for about 3 days after surgery
Vocal cord stripping Stripping of the cord is used to treat dysplasia (abnormal development), hyperkeratosis (is thickening of the stratum corneum (the outermost layer of the epidermis), often associated with the presence of an abnormal quantity of keratin,)and leukoplakia It involves removal of the mucosa of the edge of the vocal cord using operating microscope
Cordectomy Excision of the vocal cord via transoral laser Laser surgery Have several advantages Treatment and recovery are shorter, with few side effects and less costly Microelectrodes are useful for surgical resection Carbon dioxide laser can be used for the treatment of many laryngeal tumors
Total laryngectomy When cancer of the larynx is advanced total laryngectomy It includes removal of the epiglottis, thyroid cartilage, hyoid bone, cricoid cartilage and three or four rings of the trachea The pharyngeal opening to the trachea is closed and the remainder of the trachea is brought out to the neck wound and sutured to the skin to form a permanent tracheostomy through which the patient breaths
The person has no voice because of loss of the larynx The patient loses the sense of smell because breathing through the nose is impossible Initially the person has runny nose because sniffing in and out is not possible
Radical neck dissection A radical neck dissection may be performed along with the laryngectomy when risk of metastasis to the neck is high In this the surgeon removes the submandibular salivary gland, sterno cleido mastoid muscle, internal jugular vein, and spinal accessory nerves This extensive surgery is done to prevent nodal spread. Selective, modified, conservative or functional neck dissections
Radical neck dissection causes atrophy of the trapezius muscle and the shoulder droops on the side of surgery. The physical therapist or nurse can assist patients with range of motion exercises, which will gradually replace the function of the lost muscles Mid fowlers position is best it can helps reduce facial edema, improve circulation and reduce or prevent headaches from lymphedema.
Reconstructive surgery In past skin grafts were used for reconstruction Today myocutaneous flaps and free flaps are most commonly used to reconstruct large deficits caused by extensive tumor resection
Myocutaneousflaps Myocutaneous flaps use the axial blood supply that supplies muscle mass, as well as cutaneous and subcutaneous tissue. The inclusion of muscle with its blood supply when transferring the skin allows for a much greater range of rotation of the flap The pectoralis major, latissimus dorsi, trapezius and sternocleidomastoid muslces can be used for myocutaneous flap
Free flaps It consist of harvested tissue separated from the donor site with the vein and artery. The vein and artery are anastomosed to recipient vessels close to the defect (microvascular anastomosis) Low dose aspirin or even heparin to prevent clot formation
Preoperative care Explain the patient that after total laryngecotmy the breathing will occur through a permanent opening made in the neck and that normal speech will not be possible This will leads to depression to the patient The patient should meet a speech pathologist before surgery to learn about options for post operative rehabilitation and speech In some cases, a visit from another persons who undergone same surgery can be useful
Sometimes the visit of that patient can leads to depression again, so careful assessment must be handle and fix that when the patient should meet (before or after surgery) Referring to Lost chord club or new voice club Local speech rehabilitation centers supply instructive films and other resources
Care of the patient after total laryngectomy Provide comfort care and airway management Elevate head of bed 45 degrees Encourage deep breathing every 4 hours Assess airway patency every shift as needed Maintain oxygen to tracheostomy collar Assess vitals quality, rate of respiration and skin color (pallor, cyanosis) Auscultate lungs every shift as needed
Provide care for suture line and stoma site Assess suture line and stoma site every 4 hours Report erythema, purulent drainage or hematoma Monitor drain function and output Maintain suction to drain at level ordered Milk tubing every 1 to 2 hours for 24 hours and then every 4 hours Report changes in amount and color of drainage or air leak Clean the stoma site and suture line with hydrogen peroxide, normal saline and dry it with dry gauze.
Attention to fluid, food and hygiene needs Monitor hydration and ensure adequate fluid intake to maintain healthy oral mucosa Provide mouth care atleast three times a day Record intake and output every shift Weigh the patient daily, at the same time and in the same amount of clothing Provide stoma care every shift as needed Administer enteral feedings as ordered Assess patients tolerance to feedings Assess bowel sounds every shift as needed
Report intolerance to feedings (nausea, fullness, inability to feed) Record amount, consistency and frequency of stools Assess swallowing ability, and provide support when oral diet resumes
Provide support and education for the patient family Assess anxiety level and provide emotional support Assist patient in communicating Provide patient with writing materials or picture board Use questions that can be answered yes or no Instruct about use of artificial speech device and encourage its use Be sensitive to patients reactions to changes in appearance Provide time to listen to patient Encourage use of lost chord or new voice club
Prepare patient for discharge Begin teaching laryngectomy care Monitor ability of patient to perform airway management care Provide information about soft diet Review written instructions in home going booklet with patient and family Refer the patient to a speech pathologist for voice and speech rehabilitation
Speech rehabilitation Tracheoesophageal speech in this a tracheoesophageal puncture (TEP) is made to create a tracheoesophageal fistula large enough for insertion of a valve prosthesis. Artificial larynx or electro larynx mechanical device which create natural type of speech
Complications due to surgeries Hematoma, wound dehiscence, tissue loss, pharyngocutaneous fistula , carotid artery rupture, problems with appearances Complications of myocutaneous and free flaps includes venous or arterial congestion, flap necrosis and slough.
Regional lymph nodes (N) NX Regional nodes cannot be assessed N0 No regional lymph node metastasis N1 Metastasis in a single ipsilateral lymph node =3cm in greatest dimension N2 Metastasis in a single ipsilateral lymph node >3cm but not more than 6cm in greatest dimension; or in multiple ipsilateral lymph nodes, none >6cm in greatest dimension; or in bilateral or contralateral lymph nodes, none >6cm in greatest dimension N2a Metastasis in a single ipsilateral lymph node >3cm but not more than 6cm in greatest dimension N2b Metastasis in multiple ipsilateral lymph nodes, none >6cm in greatest dimension Metastasis in bilateral or contralateral lymph nodes, none >6cm in greatest dimension N2c N3 Distant metastasis (M) M0 M1 Metastasis in a lymph node >6cm in greatest dimension No distant metastasis Distant metastasis
Stage 0 I II III T Tis T1 T2 T3 T1 T2 T3 T4a T4a T1 T2 T3 T4a T Any T4b T Any N N0 N0 N0 N0 N1 N1 N1 N0 N1 N2 N2 N2 N2 N3 N Any N Any M M0 M0 M0 M0 M0 M0 M0 M0 M0 M0 M0 M0 M0 M0 M0 M1 IVA IVB IVC













")






























")