Management and Guidelines for Complicated Intra-Abdominal Infection (CABI)
Investigate the management challenges and existing guidelines for Complicated Intra-Abdominal Infection (CABI), including proposed trials and audits to optimize antibiotic therapy. Explore the findings of the CABI audit and service evaluation to define patient populations and pathology, presented in February 2016 for collaboration and research initiatives.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
CABI (Complicated intra-ABdominal Infection) national prospective audit & service evaluation Mr Dermot Burke, Dr Rachel Hyland, Dr Andrew Kirby, Dr Anne Melhuish, Dr Shafaque Shaikh & National Infection Trainee Collaborative for Audit and Research Yorkshire Surgical Research Collaborative
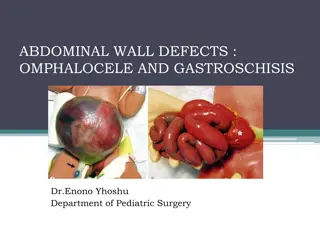
Complicated intra-abdominal infection (CABI) = infection within the abdomen where there is perforation of a viscus or a collection which is believed to be infected, e.g. Intra-abdominal abscess Perforated bowel after ischaemia Post-operative complication
CABI characteristics Occur across a wide range of specialties Associated with significant morbidity and mortality Heterogeneous in: Size, number, location, loculation, potential for drainage/washout, ongoing source e.g. anastomotic leak Treatment is based on: Source control Antibiotics
Management of CABI UK practice unknown Current practice likely to vary at: Speciality level: surgical vs. microbiologist approach Doctor level: individual doctor vs. individual doctor Patient level: mild vs. moderate vs. severe disease Management difficulties compounded by: Lack of evidence No comprehensive evidence-based guidelines
Current guidelines Existing guidelines: limited in scope largely based on expert opinion National level guidelines: Infectious Disease Society of America (IDSA): recommend 4-7 days antibiotics unless source control not achieved no comment on duration without source control Taiwanese guidelines recommend 7-10 days antibiotics where drainage is achieved, with up to four weeks of intravenous therapy, followed by a prolonged course of oral antibiotics in patients who are more ill.
Proposed trial & audit Short course ( 10 days) vs. long course (28 days) antibiotic therapy for the treatment of CABI In order to inform trial, baseline data needed CABI audit designed Presented to NITCAR February 2016 meeting, accepted as a project
CABI audit & service evaluation Multi-centre participation, each site collects data on a minimum of 7 patients Aim to: Define the patient population Define the pathology (site, type) Define the current management strategies and their successes Compare these to guidelines Define at risk populations for relapses Define outcome rates
So far... 40 sites signed up Data submitted from 4 sites Closing date for data submission = end of May 2017 Data analysis planned June to August 2017
http://nitcollaborative.org.uk/wp/projects-cabi/ Email: cabi@leeds.ac.uk
")
 =")