Managing Epidemics: Key Facts on Deadly Diseases and Emerging Threats
Explore the re-emergence of infectious diseases, the impact of new pathogens, and the global epidemic events from 2011 to 2017. Discover the history of deadly diseases, including Ebola, HIV, and more, and learn how history might repeat itself in the face of future outbreaks.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
VERSION 1 Managing epidemics Key facts about major deadly diseases
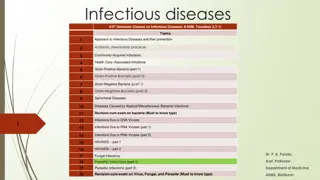
P ART I 14 MANAGING EPIDEMICS | KEYFACTSABOUT MAJOR DEADLYDISEASES The re-emergence of infectious diseases The threat continues New Infectious Threats continue to Emerge Infectious Diseases don t go away. Since 1970, more than 1,500 new pathogens were discovered, 70% proved to be of animal origin: a connection that deserves renewed scrutiny. Not all of them have had a public health impact but some of them have become famous. They included the Ebola virus, Ebola has surfaced in almost 25 separate and deadly outbreaks, Human immunodeficiency virus (HIV), HIV, infected about 70 million people in just 35 years, killed an estimated 35 million people in the same period.
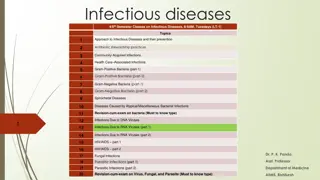
Epidemicevents* globally, 20112017**:A total of 1,307 epidemic events Number of epidemic events* by diseaseand year TOTAL Yellow fever 17 12 8 2 4 10 4 57 Chikungunya 8 10 3 29 27 14 4 95 Viral haemorrhagic fever 6 4 10 Ebola virus disease 1 2 11 4 3 1 22 Marburg virus disease 1 1 2 4 Crimean-Congohaemorrhagic fever 3 5 6 8 7 7 13 49 Rift Valley fever 1 1 1 1 1 4 5 14 Cholera 62 51 47 37 44 42 25 308 Typhoid fever 20 23 5 2 8 3 14 75 Shigellosis 25 24 28 29 4 2 1 113 Plague 8 7 6 10 7 6 3 47 Lassa fever 2 1 2 3 2 7 6 23 WestNile fever 11 15 15 11 11 18 10 91 Zika virus disease 5 7 19 54 52 137 Meningitis 14 20 19 19 19 23 23 137 MERS-CoV 3 10 17 12 7 8 57 5 6 7 9 10 5 9 51 Influenza A Monkeypox 2 2 5 10 Nodding syndrome 1 1 2 Nipah virus infection 1 1 1 1 1 5 2011 2012 2013 2014 2015 2016 2017** * Analysis excluded Poliomyelitis. The following epidemic and pandemic diseases were analysed: Avian Influenza A(H5N1), A(H7N9), A(H7N6) A(H10N8), A(H3N2), A(H5N6), A(H9N2), Chikungunya, Cholera, Crimean-Congo haemorrhagic fever, Ebola virus disease, Lassa fever, Marburg virus disease, Meningitis, MERS-CoV, Monkeypox, Nodding syndrome, Nipah virus infection, Plague, Rift Valley fever, Shigellosis, Typhoid fever, Viral haemorrhagic fever, West Nile fever, Yellow fever, Zika virus disease. If a disease caused more than 1 epidemic event by year in a country, it was only counted once for the year it occurred in that country. Includes cases imported or locally transmitted. Source: data reported to WHO and in media ** WHO/IHM data as of 12 January 2018 (note: 2017data is not complete) P ART I 23 MANAGING EPIDEMICS | KEYFACTSABOUT MAJOR DEADLYDISEASES
Will history repeat itself? Yes, it will. Whether transmitted by mosquitoes, other insects, contact with animals or person-to-person The only major uncertainty is when they, or something equally lethal, will arrive. What are we doing about it?
The 21st century: already a long series of scourges Deeply scarred by so many major epidemics. Take the plague, .A thing of the past? A major outbreak in Madagascar in 2017 led to a total of at least 2,417 confirmed, probable and suspected cases, including 209 deaths. Diseases very rarely disappear.And there always seems to be room for new ones. SARS Severe acute respiratory syndrome affected more than 8,000 people, killing about one in ten of them, causing fear and panic across the world, and inflicting enormous economic damage,. P ART I 15
Faster and further with a greater impact Localized can now become global very rapidly For example, the influenza pandemic of 2009 reached all continents in less than nine weeks. In 2015, one traveler returning home to the Republic of Korea from spending time in the Middle East brought MERS back with him. The consequences: AKorean outbreak, 186 cases, 36 deaths, and outbreak-related losses of approximately US$ 8 billion, all in the space of two months. Spread more widely and more quickly, ruinous impact on the economy of the affected country and spill over into to the global economy, disrupting travel, trade and livelihoods. P ART I 17 MANAGING EPIDEMICS | KEYFACTSABOUT MAJOR DEADLYDISEASES
P ART I 18 MANAGING EPIDEMICS | KEYFACTSABOUT MAJOR DEADLYDISEASES Ready and able to detect the next outbreak Given the effects of globalization, the intense mobility of human populations, and the relentless urbanization Initial Delay in Recognizing Serious impact on Travel and Trade Public Reaction Anixiety Panic and Confusion Media Coverage Global health security depends crucially on Awareness Cooperation Collaboration Improve early detection TheEbola outbreakundiagnosed for more than two months. virus to spread unseen, capitalcities where the outbreaks grew into largeepidemics.
Increasing health security is preparedness. Adapt to any novel (new) agent, Known pathogens How will they behave, mutate Fear of the unknown Out of proportion to the real threat Inadequate decisions Inappropriate behaviours Risk Communication is critical Social Political Economic Impact Known epidemics: still a severe threat Polio Measles Mumps Strengthening health systems: essential in epidemics
Challenges and risk factors for 21st century epidemics New lifestyles spread diseases further Increase Contact between people, animals Fast Intense mobility International Travel Mega Cities Major Transport Hubs Migration from Rural to Urban Increased Trade Refuges Asylum Seekers Economic migrants P ART I 25 MANAGING EPIDEMICS | KEYFACTSABOUT MAJOR DEADLYDISEASES
Epidemic phases and response interventions Early detection interventions Controland mitigation Eliminationor eradication Response Anticipation Containment Epidemic phases Introductionor emergence Localized transmission Reduced transmission Amplification P ART I 29
Information on COVID-19 is rapidly changing, sometimes daily. Refer to reliable sources such as the CDC, OSHA, NIOSH, State Health Departments and peer reviewed science publications. 12
What can individuals do? Be informed and prepared. Wear a mask. Maintain social distancing (6 feet). Wash your hands frequently. Use alcohol-based hand sanitizer. Avoid touching your eyes, nose, and mouth. Stay home when you are sick. Cough or sneeze into a tissue or your elbow. Clean and disinfect frequently touched objects and surfaces such as cell phones. 13
What is SARS-CoV-2? SARS-CoV-2 is the virus that causes coronavirus disease 2019 (COVID-19) SARS = severe acute respiratory distress syndrome Spreads easily person-to-person Little if any immunity in humans Detailed information: https://www.cdc.gov/coronavirus/2019- ncov/index.html 15
Transmission COVID-19 is spread from person to person mainly through coughing, sneezing, and talking and breathing. Droplet - respiratory secretions from coughing or sneezing landing on mucosal surfaces (nose, mouth, and eyes) Aerosol - a solid particle or liquid droplet suspended in air Contact -Touching something with SARS-2 virus on it and then touching mouth, nose or eyes Other possible routes: Through fecal matter 16
COVID-19 can cause mild to severe symptoms Other symptoms may include: Sore throat Runny or stuffy nose Body aches Headache Chills Fatigue Gastrointestinal: diarrhea, nausea Loss of smell and taste Most common symptoms include: Fever Cough Shortness of breath 17
Severe symptoms emergency warning signs for COVID-19 Most people will have mild symptoms and should recover at home and NOT go to the hospital or emergency room. Get medical attention immediately if you have: Difficulty breathing or shortness of breath. Persistent pain or pressure in the chest. New confusion or inability to arouse. Bluish lips or face. 18
How long does SARS-CoV-2 survive outside of the body? It is not clear yet how long the coronavirus can live on surfaces, but it seems to behave like other coronaviruses. Virus may persist on surfaces for a few hours or up to several days, depending on conditions and the type of surface. It is likely that it can be killed with a simple disinfectant on the EPA registered list below. https://www.epa.gov/pesticide-registration/list-n-disinfectants-use-against-sars-cov-2 19
Increased risk of severe illness COVID-19 poses a greater risk for severe illness for people with underlying health conditions: Heart disease Lung disease such as asthma Diabetes Suppressed immune systems The elderly have higher rates of severe illness from COVID-19. Children and younger adults have had less severe illness and death. Because COVID-19 is new, there are a lot of scientific unknowns such as the impact on pregnant women and their fetuses. 20
Seasonal flu vs. COVID-19 COVID-19 has the potential to cause more deaths and hospitalizations SARS-CoV-2 is much more infectious and spreads faster than the seasonal flu 21
Pandemic influenza Experts have been recommending preparedness, warning about the likelihood of future pandemic influenzaoutbreaks for decades. Flu pandemic fatalities, worldwide, in the last century: 1918 between 40 and 100 million 1957 2 million 1968 1 million 22
Protecting workers Start with the most effective method to protect workers. Physically remove the hazard Replace the hazard Isolate people from the hazard Change the way people work Protect the worker with Personal Protective Equipment 23
Engineering controls Ventilation Drive-thru service Plastic shields and other barriers Sneeze guards 24
Administrative controls and work practices to reduce exposure Enable sick workers to stay home Establish work from home policy Minimizing contact among workers and clients Discontinue non-essential travel Limiting the number of staff present for high potential exposure tasks Training 25
Additional administrative controls Soft barriers include use of tables, ropes, signs, and floor markings to maintain social distancing. 26
OSHA PPE standard Where applicable, the OSHA PPE standard requires employers to: Conduct an assessment for PPE Provide PPE at no cost, appropriate to the hazard Train employees on how to don (put on) and doff (take off) PPE Train workers to maintain, store, and replace PPE Provide medical evaluation and fit testing 27 https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_id=9777&p_table=STANDARDS
Decontamination Employers should develop site specific decontamination procedures. Depending on the workplace, decontamination may require consultation with the health department or use of a consultant specializing in environmental cleanup. Use of an EPA registered disinfectant effective is recommended. Worker and building occupant protection is essential to protect against the virus and adverse effects of the disinfectant. EPA List: https://www.epa.gov/pesticide-registration/list-n-disinfectants-use- against-sars-cov-2 28
Respirators Respirators are needed when there is a potential for aerosol transmission. An N95 respirator is the minimum level of protection to prevent inhaling coronavirus. 29
Respirators (continued) Advantages of reusable respirators: Durability Stand up to repeated cleaning & disinfection Maintain fit over time Cost savings Powered air-purifying respirator (PAPR) Half or full-face elastomeric respirators 30
Respirators (continued) Surgical masks are not respirators! Surgical masks do not: Fit tightly against the skin to form a seal Filter tiny particles, such as viruses or bacteria that are in the air 31
Respiratory protection standard Respiratory programs must comply with all elements of OSHA Standard 29 CFR 1910.134 Written program Selection according to hazard Medically fit to wear Fit testing Ensure proper use of respirators Respirator maintenance Labeling/color coding filters Employee training Program evaluation Recordkeeping 32
PPE for jobs with high potential exposure Face/eye protection Gloves Gowns Respirators At least N95 PAPR or full or half face elastomeric for greater protection NOTE: there is a worldwide shortage of PPE! 33
Training and drills Must be hands-on and frequent Should not be primarily computer based or lecture Must include an opportunity to drill the actual process of donning and doffing PPE and respirators Should include a trained observer Cover site specific decontamination procedures. 34
Prevention in all work settings Wash hands after removing gloves or when soiled. Wear a mask. Keep common surfaces such as telephones, keyboards clean. Avoid sharing equipment if possible. Minimize group meetings by using phone, email, and avoid close contact when meetings are necessary. Consider telework. Limit unnecessary visitors to the workplace. Maintain your physical and emotional health with rest, diet, exercise, and relaxation. 35
Protection of essential workers Fire, police, grocery stores, gas stations, utilities, communications, and health care facilities are examples of essential industries and operations that remain open during a pandemic shutdown. A site and job task specific risk assessment should be conducted to document the necessary protective measures. Social distancing measures include use of barriers, signs, modifying work procedures that require close human interaction. Other steps include increased cleaning and disinfection, use of PPE and respirators, and training. 36
Mental health and stress As the number of cases of COVID-19 increase, so does the associated anxiety and stress. Consider the following steps: Use your smart phone to stay connected to family and friends. Shift from texting to voice or video calling to feel more connected. Keep comfortable. Do more of the things you enjoy doing at home. Practice stress relief whenever you feel anxiety building do some deep breathing, exercise, read, dig in the garden, whatever works for you. Avoid unhealthy behavior such as excess drinking that will just increase your anxiety afterwards. Keep looking forward. Think about plans you d like to make down the road. 37
The Role of the Vaccine Cases of COVID-19 will decrease with the administration of the vaccine. With uptake of the vaccine and continued workplace controls in place, occupational exposures will decrease. People who are vaccinated can still be exposed and potentially expose someone else even if they don t become sick. A continued focus on maintaining workplace preventive measures is important to protect workers in all industries. 38
VACCINATIONS ~ PROTECT YOURSELF & SOCIETY
COVID-19 Emergency Temporary Standard (ETS) Healthcare 29 CFR 1910.502 Employee Training Presentation June 2021
Overview of COVID-19 ETS (29 CFR 1910.502) As part of OSHA s commitment to protect workers and deliver stronger worker safety protections, the agency has issued a COVID-19 Healthcare ETS that establishes new requirements to protect workers from exposure to COVID-19 in all settings, with some exceptions, where any employee provides healthcare or healthcare support services. The ETS requires employers to: Conduct a hazard assessment and implement a COVID-19 plan for each workplace. Engage employees in the development of the plan. Designate workplace safety coordinator(s), knowledgeable in infection control principles and practices, with authority to implement, monitor, and ensure compliance with the plan. Limit and monitor points of entry to settings where direct patient care is provided; screen and triage patients, clients, residents, delivery people and other visitors and non-employees entering the setting for symptoms of COVID-19; and implement patient management strategies. Develop and implement policies and procedures to adhere to Standard and Transmission-Based Precautions in accordance with Centers for Disease Control (CDC) guidelines. Continued on next page
Overview of COVID-19 ETS (29 CFR 1910.502) Provide and ensure employees wear facemasks when indoors and when occupying a vehicle with other people for work purposes; provide and ensure employees use respirators and other personal protective equipment (PPE) for exposure to people with suspected or confirmed COVID-19 and for aerosol-generating procedures (AGPs) on a person with suspected or confirmed COVID-19; and provide respirators and other PPE in accordance with Standard and Transmission-Based Precautions. Perform AGPs on persons with suspected or confirmed COVID-19 in an airborne infection isolation room, if available; limit employees present to only those essential; and clean and disinfect surfaces and equipment promptly after the procedure is completed. Keep employees at least 6 feet apart from others when indoors, unless not feasible for a specific activity (e.g., hands-on medical care). Install cleanable or disposable solid barriers at fixed work locations in non-patient care areas where employees are not separated from other people by at least 6 feet. Follow standard practices for cleaning and disinfection of surfaces and equipment in accordance with CDC guidelines in patient care areas, resident rooms, and for medical devices and equipment or in all other areas when a person who is COVID-19 positive has been in the workplace in the last 24 hours; in all other areas, clean high-touch surfaces and equipment at least once a day; and provide alcohol- based hand rub that is at least 60% alcohol or provide readily accessible handwashing facilities. Continued on next page
How to Safely Don, Use, and Remove PPE
Key Points About PPE Don before contact with the patient, generally before entering the room Use carefully don t spread contamination Remove and discard carefully, either at the doorway or immediately outside patient room; remove respirator outside room Immediately perform hand hygiene
Sequence* for Donning PPE Gown first Mask or respirator Goggles or face shield Gloves *Combination of PPE will affect sequence be practical
How to Don a Gown Select appropriate type and size Opening is in the back Secure at neck and waist If gown is too small, use two gowns Gown #1 ties in front Gown #2 ties in back





























")
")













")
")