Maxillary Sinus Disease
Maxillary sinus disease, a common condition, is often linked to viral infections. Learn about the anatomy of paranasal sinuses, symptoms of acute sinusitis, and clinical features associated with maxillary sinus disease.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Maxillary antrum disease Dr.Mohammed Alaraji B.D.S.F.I.B.M.S
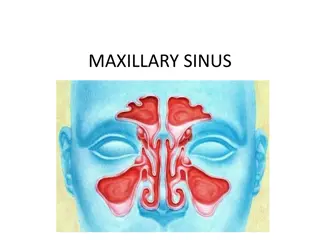
The paranasal sinuses are air-filled extensions of the nasal cavity. There are four paired sinuses named according to the bone in which they are located maxillary, frontal, sphenoid and ethmoid. Each sinus is lined by a ciliated pseudostratified epithelium, interspersed with mucus-secreting goblet cells. The function of the paranasal sinuses is a topic of much debate. Various roles have been suggested: 1. Lightening the weight of the head 2. Supporting immune defence of the nasal cavity 3. Humidifying inspired air 4. Increasing resonance of the voice
There are two frontal sinuses located within the frontal bone of the skull. They are the most superior of the paranasal sinuses, and are triangular in shape. Drainage is via the frontonasal duct. It opens out at the hiatus semilunaris, within the middle meatus of the nasal cavity. The sphenoid sinuses are situated within the body of the sphenoid bone. They open out into the nasal cavity in an area supero-posterior to the superior cocha known as the spheno-ethmoidal recess. There are three ethmoidal sinuses located within the ethmoid bone: 1. Anterior Opens onto the hiatus semilunaris (middle meatus) 2. Posterior Opens onto the lateral wall of the superior meatus 3. Middle Opens onto the lateral wall of the middle meatus
The maxillary sinus is located under the eyes in the maxillary bone. Adjacent structures include the lateral nasal wall, the orbital floor, and the posterior maxillary wall which contains the pterygopalatine fossa. The maxillary sinus is innervated by the infraorbital nerve (CN V2). The maxillary and facial arteries supply the sinus, and the maxillary vein supplies venous drainage.
ACUTE SINUSITIS Acute maxillary sinusitis is a very common condition that often presents with pain suggesting a dental cause. However, almost all acute sinusitis is a sequela of viral infection in the nasal passages and sinuses. Inflammation inhibits mucociliary clearance, and oedema restricts sinus drainage by narrowing the ostium, raising the internal pressure.
Clinical features Onset almost always follows a respiratory viral illness. Infection of the lining mucosa is by the same virus that caused the respiratory infection and usually resolves with the main infection in 7 10 days. Symptoms lasting longer probably indicate bacterial infection. There is sudden onset of pain from the sinus, often poorly localised, with tenderness of the overlying skin. Teeth with roots in or close to the antrum are painful on pressure. There are also nasal congestion, weakened sense of smell and sometimes referred pain to the ear. Fluid will often discharge into the nose on tilting the head or lying down and movement of the head worsens pain. Involvement of ethmoid or sphenoid sinuses is often perceived by patients as headache high-dose amoxicillin or amoxicillin with clavulanic acid are appropriate empirical first-line drugs. If these fail, a pus sample for sensitivity testing must be obtained by puncture of the sinus.
CHRONIC SINUSITIS Chronic sinusitis may develop with or without a preceding acute sinusitis. The clinical features are those of the acute disease but milder and without the generalised symptoms of upper respiratory tract viral infection. When pain is poorly localised, radiographic examination of the sinuses may reveal mucosal thickening, mucosal polyps or a fluid level. CT scan is the examination of choice , but the maxillary antrum is well visualised on panoramic tomography or occipitomental view. Chronic sinusitis in some patients produces nasal polyps, oedematous thickenings and pedunculated polyps of the mucosa. These can fill the lumen, block drainage and cause persistence of sinusitis.
Management Patients with chronic sinusitis without a dental cause must be referred to a specialist. Polyps, allergic and fungal causes must be excluded by endoscopy. Antibiotic treatment alone usually fails and a combined approach with improving drainage, saline irrigation, reducing inflammation with topical steroids and tackling infection is required. Endoscopic sinus surgery may be required if there is no improvement in a few weeks.
Fungal sinusitis Fungal sinusitis results from inhalation and germination of air-borne fungal spores that are not cleared by mucociliary transport, usually because of pre-existing sinus inflammation. Mucormycosis, also known as black fungus is a serious fungal infection, usually in people with reduced ability to fight infectionsSymptoms depend on where in the body the infection occurs It most commonly infects the nose, sinuses, eye and brain resulting in a runny nose, one sided facial swelling and pain, headache, fever, blurred vision, swollen and bulging eye, and tissue death
Risk factors include diabetes with persistently high blood sugar levels or diabetic ketoacidosis, low white cells, cancer, organ transplant, iron overload, kidney problems, long-term steroids or immunosuppressant use, and to a lesser extent in HIV/AIDS. Diagnosis is by biopsy and culture, with imaging to help determine the extent of disease. Treatment is generally with amphotericin B and surgical debridement. During the COVID-19 pandemic 2020/21, an association between mucormycosis and COVID-19 has been reported following treatment and recovery from COVID-19. Surgery can be very drastic, and in some cases of disease involving the nasal cavity and the brain, removal of infected brain tissue may be required. Removal of the palate, nasal cavity, or eye structures can be very disfiguring.[Sometimes more than one operation is required.
SURGICAL DAMAGE TO THE MAXILLARY ANTRUM The floor of the antrum may be damaged during dental extractions that cause an oroantral communication. If the antrum is opened during an extraction, a displaced root or bacteria from the mouth can introduce infection If sinusitis becomes established and the fistula has not been closed, the walls of the passage may become epithelialised, polyps develop in the sinus mucosa and the opening becomes a permanent fistula.
Displacement of a root or tooth into the maxillary antrum A tooth or root can be driven into the antrum if excessive force has been used during extraction or in attempting to elevate fragments, particularly when a thin antral floor extends down into the alveolar ridge.
Management The position of the root or tooth should be confirmed. Sometimes it is still within the alveolar process or between the mucosal lining and bony floor. If the fragment is not visible on a periapical radiograph and occlusal view, cone beam CT provides the best localisation. Plain films taken with the head in two different positions will reveal whether the tooth is mobile. After any acute sinusitis has been treated, the surgical approach depends on the position of the root and whether there is a wide oroantral opening. The classical method is to reflect a mucoperiosteal flap in the labiobuccal sulcus, open the antrum in the canine fossa (Caldwell Luc approach) and find the root by direct vision or endoscopy.
The tooth or fragment may then be removable on a sucker nozzle. A more conservative approach without the need for wide external surgical access is by functional endoscopic sinus surgery, which preserves the sinus ciliary transport, improves drainage after the operation and causes less morbidity.
Oroantral communication The usual test for communication is to ask the patient to blow gently against pinched nostrils. Air (detectable with a tuft of cotton wool held in tweezers), blood, pus or mucus will then be expelled from the opening into the mouth. if the communication is small, or only suspected, this can cause more damage or even produce a communication. In such cases it is better to pack and suture the socket and allow a period of healing during which the patient must avoid nose blowing and use nasal decongestants and antibiotics. Definite or large communications are best closed immediately surgically.
Buccal advancement flap E xcise fistula (and submit for histology) or use as superior layer by placing a purse- string suture, and raise a wide- based buccal flap over bone. Incise the periosteum along the length of the flap to allow the mucosa to advance over the socket. Close over bone without tension and suture to palatal mucosa. Mattress sutures can be helpful. Postoperative antibiotics/ decongestant/ menthol/ analgesia. Buccal fat pad flap buccal advancement flap, the buccal pad of fat is often exposed. Mobilize the fat and use it to provide a two- layered closure Palatal advancement flap E xcise fistula (use as stated if possible) and raise a full- thickness mucoperiosteal palatal flap based on the palatine artery rotate over the socket and suture. Bare bone in the palate left to granulate under a cover plate.
CARCINOMA OF THE ANTRUM Carcinoma of the maxillary antrum is rare. Pain is not an early symptom, and a large size can be attained before presentation. Later, pain and anaesthesia in the distribution of adjacent nerves develop. Most are squamous and often poorly differentiated; some are adenoid cystic carcinomas arising in the mucosal glands. Spread to vital structures around the base of the skull is often present on diagnosis. Oral and dental symptoms from carcinoma of the antrum result from involvement of its floor. This may cause pain in the teeth or under a denture. As the disease advances, teeth may become loose and a swelling becomes obvious.Any dental radiograph from a person older than 40 years showing an opaque maxillary antrum or erosion of the antral wall without obvious underlying dental or nasal disease indicates a need for further investigation.