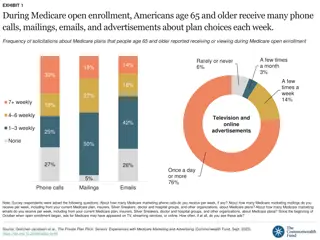
Medicare Claims for Cardiovascular Outcomes in Women's Health Initiative
This presentation discusses the effectiveness of Medicare claims in identifying cardiovascular outcomes in participants of the Women's Health Initiative. Dr. Dale Burwen from the National Heart, Lung, and Blood Institute presents findings analyzed by Dr. Garnet Anderson from the WHI Clinical Coordinating Center at the MESA Steering Committee Meeting in April 2013.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
How Well Do Medicare Claims Identify Cardiovascular Outcomes in the Women s Health Initiative? Dale Burwen, MD, MPH National Heart, Lung, and Blood Institute Presented by Garnet Anderson, PhD WHI Clinical Coordinating Center MESA Steering Committee Meeting April 24-26, 2013
Acknowledgements WHI CMS Implementation WG Garnet Anderson Mary Pettinger Ross Prentice Marian Limacher Karen Margolis Beth Virnig CCC analysts CHD WG Mark Hlatky Roberta Ray Matthew Allison Timothy Assimes Anthony Bavry Jeffrey Berger Rhonda Cooper- DeHoff Susan Heckbert Karen Johnson Anna Kucharska- Newton Wenjun Li Simin Liu JoAnn Manson Karen Margolis Lisa Martin Marco Perez Jennifer Robinson Monika Safford Marcia Stefanick Hillary Tindle Wolfgang Winkelmayer STROKE WG Kamakshi Lakshminarayan Joseph Larson Beth Virnig Norrina Allen Marian Limacher Monika Safford Wolfgang Winkelmayer PAD WG Matthew Mell Mary Pettinger Golareh Agha Matthew Allison Michael Criqui Susan Heckbert Mark Hlatky JoAnn Manson Lisa Martin VTE WG Dominic Cirillo Chunyuan Wu Matthew Allison Jeffrey Berger Charles Eaton Matthew Freiberg Elizabeth Habermann Marian Limacher Karen Margolis Jennifer Robinson Monika Safford Robert Wallace HSR SIG Karen Margolis NHLBI Jacques Rossouw Abbreviations: CHD, coronary heart disease; CMS, Centers for Medicare & Medicaid Services; HSR SIG, Health Services Research Scientific Interest Group; PAD, peripheral artery disease; VTE, venous thromboembolism; WG, working group 2
Outline Background Women s Health Initiative (WHI) Medicare Validation Effort Agreement Between WHI and Medicare Data Methods Preliminary Results (Stroke, CHD, PAD, VTE) Applications CHD hormone trial analysis VTE incidence analysis 3
Background: WHI To identify strategies for preventing chronic diseases in postmenopausal women which are the major causes of death, disability and frailty 161,808 women ages 50-79 enrolled 1993-1998 68,132 in Clinical Trials (CT) - Hormone Therapy Trials (HT) - Dietary Modification Trial (DM) - Calcium/Vitamin D Trial (CaD) 93,676 in Observational Study (OS)
WHI now 93,558 TOTAL 1 Observational Study Medical Records Cohort (24%) (AA, Hispanic, HT women) 22,313* ** 8,000 Long Life Study (age >63) *Self-report followed by documentation and central adjudication+CMS+NDI **Self-report+CMS+NDI (except cancer fully documented)
Medicare Validation Effort Adjudication of cardiovascular outcomes limited to a quarter of participants starting in 2010 Key outcomes increase substantially with age, outpacing resources for medical record review Medicare data can potentially provide outcome data on a large proportion of WHI participants Validation effort initiated to assess whether Medicare data can be used for cardiovascular outcomes in WHI Identify useful coding algorithm Assess and publish algorithm performance 6
Agreement Analysis: Methods Four projects contributed to the comparison; others planned CHD, Stroke, PAD, VTE Study population WHI participants in fee-for-service Medicare at baseline (1993-1998) - Some analyses also included participants who aged in Excluded participants who had WHI outcome of interest prior to entering Medicare Medicare data through 2007 or 2010 Project specific cohorts selected based on availability of WHI adjudicated outcomes and other factors Divided into training and test sets Coding algorithms Evaluated and modified as needed in training set Used hospital claims (MedPAR file) and ICD-9-CM discharge diagnoses and procedure codes Some analyses also used CPT/HCPCS codes from Carrier/Outpatient claims files 7
Agreement Analysis: Methods (cont.) Performed person-based analysis Assessed agreement Kappa statistic Sensitivity (SN), specificity (SP), positive predictive value (PPV), negative predictive value (NPV) - WHI diagnosis defined as gold standard Assessed reasons for disagreement Additional analyses excluded records that were not informative with regard to performance of Medicare data E.g., WHI medical record not received 8
Training Set Results: Stroke Stroke (any diagnosis position) All WHI Yes No 505 240 77 23606 CMS Yes No WHI strokes = 582 (~100% true) CMS strokes = 745 (how many true?) 9
Interval Between WHI and CMS Event 505 participants had stroke in WHI and CMS 83% on same date 88% within +/- 1 day 91% within +/- 3 days 95% within +/- 7 days 96% within +/- 30 days Range* -4269 to 682 days * WHI date CMS date 10
Training Set Results: Stroke Stroke (any diagnosis position) All WHI SN (%) 87 PPV (%) 68 Kappa Yes No 505 240 77 23606 CMS Yes No 0.75 SP = 99%; NPV = >99% SN, sensitivity; SP, specificity; PPV, positive predictive value; NPV, negative predictive value 11
Training Set Results: Stroke Stroke (any diagnosis position) All WHI SN (%) 87 PPV (%) 68 Kappa Yes No 505 240 77 23606 505 125 73 23606 505 65 73 23606 CMS Yes No CMS Yes No CMS Yes No 0.75 WHI hospitalization reported* WHI hospitalization adjudicated 87 80 0.83 87 89 0.88 * Excludes strokes managed in the outpatient setting only. Also, excludes discordant events for which no WHI hospitalization was reported within +/- 30 days of the Medicare admission. Excludes discordant events for which WHI stroke adjudication was planned but no medical records were received, as well as events for which no stroke adjudication was attempted. SN, sensitivity; PPV, positive predictive value 12
Interim Summary 1 Stroke date mostly same in WHI and CMS data Longer intervals may be date errors or separate events Although WHI diagnosis defined as gold standard , ascertainment of hospitalizations was imperfect Key reason for a CMS event without WHI match was lack of WHI report of hospitalization E.g., Inadequate recall, disability/death and lack of proxy report Even if hospitalization reported to WHI, it was not necessarily adjudicated by the stroke committee E.g., No medical records received; records reviewed by another committee only; reported reason for hospitalization did not trigger stroke review. Limiting analysis to CMS events that could be evaluated with WHI adjudicated records increased PPV 13
Various Outcomes: PPV PPV (%) Stroke MI CABG PCI VTE Car otid 81 AAA LE PAD 58 All 68 71 89 86 62 63 WHI hospitalization reported* WHI hospitalization adjudicated 80 81 94 94 72 92 67 73 89 86 95 95 91 94 74 82 * Participants with CMS-only events were excluded if no WHI hospitalization reported within +/-30 days. Participants with CMS-only events were excluded if no WHI hospitalization adjudicated within +/-30 days. Further evaluation by reviewing CMS physician claims and selected medical records yielded PPV estimate of 91%-94% for AAA and 92%-95% for LE PAD. Stroke (any diagnosis position); MI, myocardial infarction (any diagnosis position; WHI clinical MI); VTE, venous thromboembolism (pulmonary embolism or deep venous thrombosis [any diagnosis position]); Carotid (treatment procedure); AAA, abdominal aortic aneurysm (treatment procedure); LE PAD, lower extremity peripheral artery disease (treatment procedure) 14 Preliminary results: Please do not distribute
Various Outcomes: Sensitivity and Kappa Sensitivity (%) Stroke MI CABG PCI VTE Car otid 92 AAA LE PAD 73 All 87 79 94 90 84 90 Kappa* Stroke MI CABG PCI VTE Car otid 0.86 AAA LE PAD 0.65 All 0.75 0.74 0.91 0.88 0.71 0.74 * Kappa increased if exclude discordant events with no WHI hospitalization reported or adjudicated Stroke (any diagnosis position); MI, myocardial infarction (any diagnosis position; WHI clinical MI); VTE, venous thromboembolism (pulmonary embolism or deep venous thrombosis [any diagnosis position]); Carotid (treatment procedure); AAA, abdominal aortic aneurysm (treatment procedure); LE PAD, lower extremity peripheral artery disease (treatment procedure) 15 Preliminary results: Please do not distribute
Interim Summary 2 After limiting discordant events to those adjudicated, the PPV was Highest for certain procedures (CABG, PCI, carotid) Intermediate for MI and stroke Some AAA and LE PAD procedures found in CMS hospital data but not WHI data were corroborated by CMS physician claims or review of selected medical records (data not shown) Estimated PPV was high For VTE, larger proportion of hospitalizations reported not adjudicated More caution generalizing from subset adjudicated; best estimate of PPV may be lower Lower PPV especially due to codes in a secondary position (data not shown) Sensitivity was Highest for certain procedures (CABG, PCI, AAA, carotid) Intermediate for Stroke and VTE Lower for MI and LE PAD - For LE PAD, physician claims may augment ascertainment (data not shown) 16
Applications: CHD Hormone Trial Analysis Study population WHI HT participants age >65 at baseline Enrolled in fee-for-service Medicare Part A at baseline Intention-to-treat analysis using either WHI outcomes Medicare outcomes Until intervention stopped Outcomes Myocardial infarction (MI) Revascularization (CABG/PCI) Primary analysis pooled HT trials Estrogen alone (E-alone) Estrogen and Progestin (E+P) Hazard ratios using WHI outcomes were compared to hazard ratios using Medicare outcomes 17
CHD Hormone Trial Analysis MI WHI Medicare Pooled HT 150 127 Placebo 120 101 HR* 1.31 1.29 95%CI 1.03, 1.67 1.00, 1.68 MI WHI Medicare E-alone 76 66 Placebo 66 52 HR 1.23 1.35 95%CI 0.88, 1.71 0.94, 1.95 MI WHI Medicare E+P 74 61 Placebo 54 49 HR 1.41 1.23 95%CI 0.99, 2.01 0.85, 1.80 * Difference between hazard ratios not significant in 1000 bootstrap replications MI, WHI clinical MI (excludes silent MI); Medicare MI any diagnosis position 18 Preliminary results: Please do not distribute
CHD Hormone Trial Analysis Revasc WHI Medicare Pooled HT 181 195 Placebo 171 179 HR* 1.09 1.10 95%CI 0.88, 1.35 0.89, 1.35 Revasc WHI Medicare E-alone 107 115 Placebo 90 97 HR 1.26 1.20 95%CI 0.95, 1.67 0.92, 1.58 Revasc WHI Medicare E+P 74 80 Placebo 81 82 HR 0.91 0.97 95%CI 0.67, 1.25 0.71, 1.33 * Difference between hazard ratios not significant in 1000 bootstrap replications Revascularization, CABG/PCI 19 Preliminary results: Please do not distribute
Applications: VTE Incidence Analysis Number of participants with VTE important for incidence analysis Example using 50% HT cohort Incidence estimate may be higher using Medicare hospital claims VTE 36% higher PE 23% higher DVT 36% higher Also, some differences in the persons identified with the events Additional algorithms being tested E.g., Only count hospital DVT code if corroborated by subsequent ambulatory diagnosis or prothrombin/INR test VTE 192 261 PE 101 124 DVT 138 188 WHI Medicare 20 Preliminary results: Please do not distribute
Interim Summary 3 Relatively high agreement between WHI and Medicare data for MI, CABG, PCI Translated into similar hazard ratios in HT Caution needed with small relative risks, such as those in clinical trials E.g., point estimate 1.41 vs 1.23 Caution generalizing to other outcomes Performance of each likely specific More example applications would be useful Absolute counts more critical for incidence analysis Further work ongoing to try to improve VTE coding algorithm and increase specificity and PPV 21
Discussion WHI events are ~100% true, but there is some underascertainment This type of error may have little effect on relative risk of rare events in cohort analyses* Using Medicare data, there is both underascertainment and imperfect PPV PPV results for MI and Stroke were similar to published literature only after limiting analysis of discordant events to adjudicated records Cardiovascular procedures generally performed well CABG, PCI, Carotid, AAA, LE PAD Future validation projects: heart failure, valvular heart disease, atrial fibrillation, dementia * Copeland, et al. Am J Epidemiol. 1977:105;488-495. 22
Discussion (cont.) Limitations Not all participants have fee-for-service Medicare coverage Claims data routinely available only yearly Advantages Identify outcomes without need for participant recall Provide outcomes on an expanded sample Enable long-term monitoring at relatively low cost Record all episodes of care, including subsequent events that may not be ascertained in WHI
Extra Slides 26
Codes (Preliminary) Outcome ICD-9-CM codes* Stroke 430, 431, 433.x1, 434.x1, 436 MI 410.x0, 410.x1 CABG 36.1x, 36.2 PCI 00.66, 36.0, 36.00, 36.01, 36.02, 36.05, 36.06, 36.07 AAA (441.3, 441.4, 441.5, or 441.9) AND (38.34, 38.44, 39.25, 39.52 or 39.71) LE PAD (440.20-440.24, 440.9, 444.22, 444.81, 443.81, 443.9, 447.1, or 250.70) AND (39.50, 39.90, 00.55, 17.56, 99.10, 38.08, 38.14, 38.16, 38.18, 39.25, 39.29, 84.11, 84.12, 84.15, or 84.17) (433.10, 433.11, 433.30, or 447.1) AND (38.42, 38.12, or 00.63) Carotid VTE 415.11, 415.19, 451.11, 451.19, 451.2, 451.9, 453.1, 453.2, 453.40, 453.41, 453.42, 453.8, 453.9 * MEDPAR database Further work ongoing to test additional algorithms 27
Test Set Results: PPV PPV (%) Stroke MI CABG PCI VTE Car otid 81 AAA LE PAD 56 All 65 78 93 85 62 WHI hospitalization reported* WHI hospitalization adjudicated 78 87 95 92 94 78 72 87 91 96 95 96 84 81 * Participants with CMS-only events were excluded if no WHI hospitalization reported within +/-30 days. Participants with CMS-only events were excluded if no WHI hospitalization adjudicated within +/-30 days. Stroke (any diagnosis position); MI, myocardial infarction (any diagnosis position; WHI clinical MI); VTE, venous thromboembolism (pulmonary embolism or deep venous thrombosis [any diagnosis position]); Carotid (treatment procedure); AAA, abdominal aortic aneurysm (treatment procedure); LE PAD, lower extremity peripheral artery disease (treatment procedure) 28 Preliminary results: Please do not distribute
Test Set Results: Sensitivity and Kappa Sensitivity (%) Stroke MI CABG PCI VTE Car otid 92 AAA LE PAD 76 All 87 79 95 86 71 Kappa* Stroke MI CABG PCI VTE Car otid 0.86 AAA LE PAD 0.64 All 0.74 0.77 0.94 0.85 0.66 * Kappa increased if exclude discordant events with no WHI hospitalization reported or adjudicated Stroke (any diagnosis position); MI, myocardial infarction (any diagnosis position; WHI clinical MI); VTE, venous thromboembolism (pulmonary embolism or deep venous thrombosis [any diagnosis position]); Carotid (treatment procedure); AAA, abdominal aortic aneurysm (treatment procedure); LE PAD, lower extremity peripheral artery disease (treatment procedure) 29 Preliminary results: Please do not distribute
Agreement Analysis: Cohorts* Algorithm Development Algorithm Testing Other Planned Analysis Include Aged In (Yes/No) No Medicare Parts required A CHD OS DM (not HT) OS 50% DM (not HT), OS subset HT HT Stroke OS 50% HT, OS subset --- Yes A & B PAD HT, OS subset ; hormone therapy analysis OS, DM (not HT) incidence, recurrence, mortality, risk factors Yes A & B VTE HT 50% HT 50% Yes A & B * Cohorts for algorithm development selected based on availability of WHI adjudicated outcomes, separation from planned analyses where possible, and rarity of outcome. Algorithm testing, same cohort as combined HT/OS hormone therapy analysis; algorithm development, separate cohort 30
CHD Hormone Trial Analysis MI (10) WHI Medicare Pooled HT 130 111 Placebo 105 82 HR* 1.28 1.38 95%CI 0.99, 1.66 1.03, 1.83 MI (10) WHI Medicare E-alone 66 54 Placebo 57 41 HR 1.23 1.39 95%CI 0.87, 1.76 0.93, 2.09 MI (10) WHI Medicare E+P 64 57 Placebo 48 41 HR 1.34 1.36 95%CI 0.92, 1.95 0.91, 2.04 * Difference between hazard ratios not significant in 1000 bootstrap replications MI, WHI clinical MI (excluding procedure-related and silent MIs); Medicare principal diagnosis 31 Preliminary results: Please do not distribute







")














")



")