Myocarditis and Cardiomyopathy

Heart conditions like myocarditis and cardiomyopathy affect the heart muscle, with myocarditis being an acute inflammatory condition caused by various factors, such as viral infections, toxic agents, and autoimmune responses. Myocarditis can lead to complications and may present with symptoms ranging from mild to severe heart failure. Recognizing the underlying causes and manifestations of myocarditis is crucial for proper diagnosis and management.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Although the myocardium is involved in most types of heart disease, the terms myocarditis and cardiomyopathy are usually reserved for conditions that primarily affect the heart muscle.
Myocarditis: This is an acute inflammatory condition that can have an infectious, toxic or autoimmune aetiology. Myocarditis can complicate many infections in which inflammation may be due directly to infection of the myocardium or the effects of circulating toxins.
Viral infections are the most common causes, such as Coxsackie (35 cases per 1000 infections) and influenza Aand B (25 cases per 1000 infections) viruses.
Myocarditis may occur several weeks after the initial viral symptoms and susceptibility is increased by corticosteroid immunosuppression, myocardial damage and exercise. treatment, previous radiation,
Some bacterial and protozoal infections may be complicated by myocarditis; for example, approximately 5% of patients with Lyme disease (Borrelia myopericarditis, which is often associated with AV block. burgdorferi) develop
Toxic aetiologies include drugs, which may directly injure the myocardium (e.g. cocaine, lithium and anticancer doxorubicin) which hypersensitivity reaction myocarditis (e.g. sulphonamides), lead and carbon monoxide. drugs may and penicillins such cause associated as a and
Occasionally, autoimmune conditions such as systemic lupus erythematosus and rheumatoid arthritis are associated with myocarditis. The clinical picture symptomless disorder, sometimes recognised by the presence of an inappropriate tachycardia or abnormal ECG, to fulminant heart failure. ranges from a
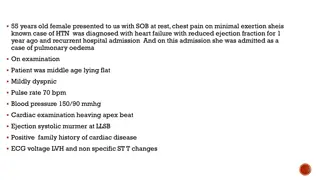
Myocarditis may be heralded by an influenza-like illness. ECG changes are common but non-specific. Biochemical markers of myocardial injury (e.g. troponin I and T, creatine kinase) are elevated in proportion to the extent of damage. Echocardiography may reveal left ventricular dysfunction that is sometimes regional (due to focal myocarditis), and if the diagnosis is uncertain it can be confirmed by endomyocardial biopsy.
In most patients, the disease is self-limiting and the immediate prognosis is excellent. However, death may occur due to a ventricular arrhythmia or rapidly progressive heart failure. Myocarditis has been reported as a cause of sudden and unexpected athletes. death in young
There is strong evidence that some forms of myocarditis may lead to chronic low-grade myocarditis or dilated cardiomyopathy; for example, in Chagas frequently recovers from the acute infection but goes on to develop a chronic dilated cardiomyopathy 10 or 20 years later. disease the patient
Specific antimicrobial therapy may be used if a causative organism however, this is rare and in most cases only supportive therapy is available. has been identified;
Treatment for cardiac failure or arrhythmias may be required and patients should be advised to avoid intense physical exertion because there is some evidence that this can induce potentially arrhythmias. There is no evidence for any benefit from treatment with immunosuppressive agents. fatal ventricular corticosteroids and
2. Cardiomyopathy: The aetiology of most intrinsic disorders of the myocardium has not been elucidated and a functional classification is used.
This impaired contraction of the LV (and sometimes the RV); left ventricular mass is increased but wall thickness is normal or reduced. Histological changes are variable but include myofibrillary loss, interstitial fibrosis and T- cell infiltrates. is characterised by dilatation and
The differential diagnosis includes coronary artery disease and some specific disorders of heart muscle, and a diagnosis of dilated cardiomyopathy should only be made when these have been excluded. The pathogenesis is not clear but dilated cardiomyopathy probably heterogenous group of conditions. encompasses a
Alcohol is an important aetiological factor in a significant proportion of patients. At least 25% of cases are inherited as an autosomal dominant trait and a variety of single gene mutations have been identified. Most of these mutations affect proteins in the cytoskeleton of the myocyte (e.g. dystrophin, lamin A and C, emerin and metavinculin) and many are associated with minor skeletal muscle abnormalities.
Most of the X-linked inherited skeletal muscular dystrophies (e.g. Becker and Duchenne) are associated with cardiomyopathy. Finally, a late autoimmune reaction to viral myocarditis is thought to be the main aetiological factor in a substantial subgroup of patients with dilated cardiomyopathy; a similar mechanism is thought to be responsible for the heart muscle disease that occurs in up to 10% of patients with advanced HIV infection.
In North America and Europe, symptomatic dilated cardiomyopathy has an incidence of 20 per 100 000 and a prevalence of 38 per 100 000. Men are affected more than twice as often as women. Most patients present with heart failure or are found to have the condition during routine investigation.
Arrhythmia, thromboembolism and sudden death are common and may occur at any stage; sporadic chest pain is a surprisingly frequent symptom. The ECG usually shows non-specific changes but echocardiography is useful in establishing the diagnosis.
Treatment is aimed at controlling the resulting heart failure. Although some patients remain well for many years, the prognosis is variable and cardiac transplantation may be indicated. Patients with dilated cardiomyopathy and moderate or severe heart failure may be at risk of sudden arrhythmic death.
This risk is substantially reduced by rigorous medical therapy with angiotensin receptor antagonists. Some patients may implantation of a cardiac defibrillator and/or cardiac resynchronisation therapy. -blockers and be considered for
This cardiomyopathy, approximately 100 per 100 000 and is characterized by inappropriate and elaborate left ventricular hypertrophy with malalignment of the myocardial fibres. is the most with common a form of of prevalence
The hypertrophy may be generalised or confined largely to the interventricular septum (asymmetric septal hypertrophy) or other regions (e.g. cardiomyopathy, a variant which is common in the Far East). apical hypertrophic
Heart failure may develop because the stiff noncompliant ventricles filling. Septal hypertrophy may also cause dynamic left ventricular outflow (hypertrophic obstructive cardiomyopathy, or HOCM) and mitral regurgitation due to abnormal systolic anterior motion of the anterior mitral valve leaflet. impede diastolic tract obstruction
Effort-related breathlessness), arrhythmia and sudden death are the dominant clinical problems. The condition is a genetic disorder, usually with autosomal dominant transmission, a high degree of penetrance and variable expression. symptoms (angina and
In most patients, it appears to be due to a single point mutation in one of the genes that encode sarcomeric contractile proteins. There are three common groups of mutation with different phenotypes. Beta-myosin heavy associated with hypertrophy. chain elaborate mutations ventricular are
Troponin mutations are associated with little, and sometimes even no hypertrophy but marked myocardial fibre disarray, an abnormal vascular response hypotension) and a high risk of sudden death. Myosin-binding protein C mutations tend to present late in life and are often associated with hypertension and arrhythmia. (e.g. exercise-induced
Symptoms and signs are similar to those of aortic stenosis, except that in hypertrophic cardiomyopathy the character of the arterial pulse is jerky.
The ECG is abnormal and shows features of left ventricular hypertrophy with a wide variety of often bizarre abnormalities (e.g. pseudo-infarct pattern, deep T-wave inversion).
Echocardiography is diagnostic, although the diagnosis may be difficult when another cause of left ventricular hypertrophy is present (e.g. physical training athletes hypertension) but the degree of hypertrophy is greater than expected. Genetic testing may facilitate diagnosis. heart,
The natural history is variable but clinical deterioration is often slow. The annual mortality from sudden death is 2 3% among adults and 4 6% in children and adolescents.
Sudden death typically occurs during or just after vigorous physical hypertrophic cardiomyopathy is the most common cause of sudden death in young athletes. Ventricular arrhythmias are thought to be responsible for many of these deaths. activity; indeed,
Beta-blockers, antagonists (e.g. verapamil) and disopyramide can help to relieve symptoms and sometimes prevent syncopal attacks; however, there is no pharmacological treatment that is definitely known to improve prognosis. rate-limiting calcium
Arrhythmias are common and often respond to treatment with amiodarone. Outflow tract obstruction can be improved by partial surgical resection (myectomy) or by iatrogenic infarction of the basal septum (septal ablation) using a catheter-delivered alcohol solution.
An ICD should be considered in patients with clinical risk factors for sudden death. Digoxin and vasodilators may increase outflow tract obstruction and should be avoided.
In this condition, patches of the right ventricular myocardium are replaced with fibrous and fatty tissue. It is inherited as an autosomal dominant trait and has a prevalence of approximately 10 per 100 000.
The dominant clinical problems are ventricular arrhythmias, sudden death and right-sided cardiac failure. The ECG typically shows a slightly broadened QRS complex and inverted T waves in the right precordial leads.
MRI is a useful diagnostic tool and is often used to screen the first-degree relatives of affected individuals. Patients at high risk of sudden death can be offered an ICD.
This disease involves the endocardium of one or both ventricles and is characterised by thrombosis and elaborate fibrosis with gradual obliteration of the ventricular cavities (e.g. endomyocardial fibroelastosis). The mitral and tricuspid valves become regurgitant.
Heart failure and pulmonary and systemic embolism are prominent features. It can sometimes eosinophilia (e.g. eosinophilic Churg Strauss syndrome). In tropical countries, the disease can be responsible for up to 10% of cardiac deaths. be associated with leukaemia,
Mortality is high at 50% at 2 years. Anticoagulation and antiplatelet therapy are usually advisable, and diuretics may help symptoms of heart failure. Surgery (tricuspid replacement with endocardium) may be helpful in selected cases. and/or decortication mitral valve the of
In this rare condition, ventricular filling is impaired because the ventricles are stiff . This leads to high atrial pressures with atrial hypertrophy, dilatation fibrillation. and later atrial
Amyloidosis is the most common cause of restrictive cardiomyopathy in the UK, although other forms of infiltration (e.g. glycogen storage diseases), idiopathic fibrosis and a familial form of restrictive cardiomyopathy do occur. perimyocyte
Diagnosis can be very difficult and requires complex Doppler echocardiography, CT or MRI, and endomyocardial biopsy. Treatment is symptomatic but the prognosis is usually poor and transplantation may be indicated.
3. Specific diseases of heart muscle: Many forms of specific heart muscle disease produce a clinical indistinguishable from dilated cardiomyopathy (e.g. connective tissue disorders, sarcoidosis, haemochromatosis, alcoholic heart muscle disease). picture that is