Non-infectious Hemodialysis Catheter Complications: Causes, Treatment Strategies
This chapter discusses catheter dysfunction, thrombus, and vein stenosis in hemodialysis patients. Explore definitions, causes, and interventions for managing non-infectious complications like catheter thrombosis and mechanical dysfunction.

Uploaded on Mar 09, 2025 | 1 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Vascular Access Education Initiative | 2015 CHAPTER 6 HEMODIALYSIS TUNNELED CATHETER NON-INFECTIOUS COMPLICATIONS AUTHORS: Lisa Miller MD, Jennifer MacRae Msc MD, Mercedeh Kiaii MD, Edward Clark MD MSc, Christine Dipchand MD Msc, Joanne Kappel MD, Charmaine Lok MD Msc, Rick Luscombe RN, Louise Moist MD MSc, Matthew Oliver MD MHSc, Pam Pike MD, Swapnil Hiremath MD MPH. On Behalf Of The Canadian Society Of Nephrology Vascular Access Work Group.
Vascular Access Education Initiative | 2015 CONTENTS Introduction Catheter Dysfunction Etiology of Catheter Dysfunction Prevention of Catheter Dysfunction Treatment of Catheter Dysfunction Central Vein Stenosis Other Complications Last Option Access Summary of Recommendations 2
Vascular Access Education Initiative | 2015 INTRODUCTION Non-infectious hemodialysis catheter complications include catheter dysfunction, catheter-related thrombus and central vein stenosis. The definitions, causes and treatment strategies for catheter dysfunction are reviewed in this chapter. Catheter-related thrombus is a less common, but serious complication of catheters, requiring catheter removal and systemic anticoagulation. In addition, the risk factors, clinical manifestation, and treatment options for central vein stenosis are outlined HD central venous catheters are associated with both infectious and non- infectious complications Occur at time of catheter insertion or at any time over the duration of catheter use Common non-infectious complications include: Catheter thrombosis Mechanical dysfunction Central vein stenosis 3
Vascular Access Education Initiative | 2015 CATHETER DYSFUNCTION Many definitions for catheter dysfunction can be found in the literature Proposed Definitions for Catheter Dysfunction High arterial pressures (<-250mmHg) High venous pressures (> 250 mmHg) High pressure alarms Decreased blood flow rates Inability to withdraw and/or flush catheter lumens Need to reverse lines Reduced urea clearance (Kt/V <1.2, or urea reduction ratio < 65%) 4
Vascular Access Education Initiative | 2015 CATHETER DYSFUNCTION NKF/DOQI defines catheter dysfunction as failure to attain and maintain an extracorporeal blood flow (Qb) of 300 mL/min at a pre-pump arterial pressure more negative than -250 mm Hg; Qb alone may not be adequate for detection of catheter dysfunction Approx. 1/3rdof tunneled catheter removal are attributed to inadequate blood flow for HD Catheter dysfunction (Qb < 300 ml/min) occurred in almost 2/3 of patients during at least one treatment; 1 catheter dysfunction per month in 30%* Interventions: instillation of thrombolytic agents; catheter exchange Consequences: disruption in the delivery of dialysis care; increase in health resource utilization * Analysis of data from DaVita dialysis facilities and US Renal Data System of HD patients receiving treatment exclusively through a catheter 5
Vascular Access Education Initiative | 2015 ETIOLOGY OF CATHETER DYSFUNCTION Early Catheter Dysfunction (likely to occur within first week post insertion) Usually a mechanical issue: Patient malpositioning Mechanical kinking of catheter (see figure 1) Incorrect catheter tip location Figure 1: 6 Courtesy of: The Atlas of Dialysis Vascular Access by Dr. Vacchharajani, esrdncc.org/wp-content/uploads/2015/12/Access-Atlas.pdf
Vascular Access Education Initiative | 2015 ETIOLOGY OF CATHETER DYSFUNCTION Early Catheter Dysfunction (occurs within first week post insertion) Catheter tip should be positioned at the junction of the superior vena cava and right atrium and confirmed with fluoroscopy Early dysfunction, especially if tip of catheter is not positioned deep enough, or touching vessel wall, should prompt consideration of catheter position Problems can sometimes be resolved by repositioning the patient or adjusting the patient s neck position, which may fix a kink or move the catheter tip away from a vessel wall 7
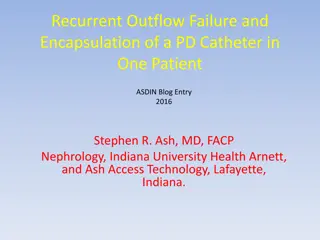
Vascular Access Education Initiative | 2015 ETIOLOGY OF CATHETER DYSFUNCTION Late (delayed) Catheter Dysfunction Occurs weeks, months or even years after the catheter has been functioning well previously Injury of vascular wall can occur at time of insertion, from manipulation or repositioning of catheter Vascular wall injury results in both turbulent blood flow and stimulation of the coagulation and inflammatory cascades Fibrin sheath (combination of fibrinogen, lipoproteins, albumin and coagulation factors) can begin to form within 24 hours of insertion or vascular wall damage (see figure 2) Sheath may partially or completed encase the catheter Leads to disturbance of catheter blood flow Associated with the development of thrombosis and infections 8
Vascular Access Education Initiative | 2015 CATHETER DYSFUNCTION : FIBRIN SHEATH Figure 2: A removed Tesio line showing a clean venous blue lower line, and a red upper line with an extensive fibrin sheath attached 9 Photo Source: Robert K. Peel, and John H. Turney Nephrol. Dial. Transplant. 2003;18:1026
Vascular Access Education Initiative | 2015 ETIOLOGY OF CATHETER DYSFUNCTION Thrombosis Occurs both in early and late catheter dysfunction; more commonly associated with late dysfunction Major contributors to thrombus formation: Intimal vessel injury Turbulent blood flow Activation of coagulation cascades Fibrin sheath formation Can occur intraluminally causing direct obstruction to blood flow Extraluminal thrombus such as right atrial or mural thrombus may cause extrinsic compression of the catheter, resulting in poor blood flow and inadequate dialysis 10
Vascular Access Education Initiative | 2015 PREVENTION OF CATHETER DYSFUNCTION Catheter instillation solutions; anticoagulant solutions Locking solutions are instilled into catheters between hemodialysis treatemtns to minimize catheter patency Sodium citrate (4%) or concentrated heparin solutions (1000 u/ml) Standard recommended locking solutions No difference in thrombolytic use or catheter removal for poor flow Consider infection prevention and local practice patterns for choice Citrate use may be associated with reduced bleeding events compared to heparin Recombinant tissue plasminogen activator (tPA) PreCLOT trial showed overall catheter malfunction was 14% decrease in catheter malfunction when tPA (1 mg in each lumen) was combined with two heparin (5000 u/ml) sessions in a thrice weekly regimen Catheter-related and all-cause bacteremia rates were also lower in tPA group vs heparin group 11
Vascular Access Education Initiative | 2015 PREVENTION OF CATHETER DYSFUNCTION Systematic Pharmacologic Therapy Antiplatelet agents e.g. aspirin, clopidogrel platelet aggregation and inhibit thrombus formation Limited conclusive evidence to recommend their use for the prevention of catheter thrombosis Potentially higher risk of bleeding should be considered Oral anticoagulants e.g. warfarin Failed to show a significant benefit in prevention of catheter malfunction Associated with a significantly higher risk of bleeding in dialysis patients 12
Vascular Access Education Initiative | 2015 TREATMENT OF CATHETER DYSFUNCTION Thrombolytic Agents and Protocols Before thrombolytic use be sure to attempt: Flushing catheter with saline Checking catheter for kinks Patient repositioning Uncertainty exists regarding best protocol for thrombolytic use Comparison of dwell vs PUSH protocols demonstrated no statistical difference of achieving a post thrombolytic blood flow 300 ml/min ALTE-DOSE study compared 1.0mg vs 2.0 mg dwell dose of tPA and found that catheter loss was significantly higher in 1mg group 13
Vascular Access Education Initiative | 2015 TREATMENT OF CATHETER DYSFUNCTION Thrombolytic Regimens Type Dose Time Delivery Non-functioning CVC (Qb < 150/200 mL/min or inability to withdraw) (short or long dwell) Typical dose: 2 mg rt- PA instillation, (1 mg in each port) 30 min after instillation (short dwell) rt-PA instilled as dwell for 30 - 60 min. Alternatives: push 1/3rd of dose every 10 min.; advance the initial pushed rt-PA at 10/15 min intervals with 0.3mL saline ; or deliver via infusion pump over 30 min. Alternative: wait additional 2 hrs (long dwell) if 30 min. fails Alternative dose: 2 mg per lumen Poor functioning CVC w dialysis stopped 2-4 mg As above As above Poor functioning CVC w dialysis ongoing (intradialytic infusion) 2-4 mg Over 1 hour Via infusion pump - delivered in the dialysis circuit with CVC lumens reversed for 30 min. then with normal positions for next 30 min. Poor functioning CVC post dialysis (lock, post HD dwell, overnight dwell) 1 - 2mg per lumen Until next dialysis rt-PA instilled as push ; allowed to dwell in catheter lumen 48-72 hrs, until next HD session 14
Vascular Access Education Initiative | 2015 TREATMENT OF CATHETER DYSFUNCTION Interventional Therapies Fibrin sheath reported to be present in 70% of catheters changed for malfunction Options Performed at time of catheter exchange to disrupt the fibrin sheath Reports of longer catheter patency, modest gains in blood flow and clearance Observational studies indicate rates of subsequent infection or catheter dysfunction post catheter exchange are on par with patients who did not have a fibrin sheath Performed using a snare or an intravascular brush Long-term data on efficacy is lacking Angioplasty (fibrin sheath plasty) Fibrin sheath stripping 15
Vascular Access Education Initiative | 2015 CENTRAL VEIN STENOSIS Occurrence rate of up to 40% in prevalent hemodialysis patients Caused by prior or current use of CVCs such as hemodialysis catheters, peripherally inserted central venous catheters (PICCs) and cardiac implantable electronic devices (CIEDs) Common sites for stenosis to occur: subclavian vein, innominate vein, cephalic arch, superior vena cava Risk Factors for central vein stenosis risk for development of central vein stenosis is associate with use of any central vein device and to some degree location of central vein device Stenosis of subclavian vein catheters occurs ~ 30-50% Internal jugular catheter stenosis occurs as high as 25-40% Indwelling CIEDs causing stenosis have been reported in 22-64% of patients Hemodialysis patients with ipsilateral arteriovenous access creation 16
Vascular Access Education Initiative | 2015 CENTRAL VEIN STENOSIS Clinical manifestations Symptoms occur as result of venous hypertension behind obstruction, though may go undetected Symptoms include: arm edema, pain and erythema from venous engorgement (with possible skin breakdown), ipsilateral breast sweelling and dilated collateral veins on upper chest, shoulder and arm Patients may develop superior vena cava syndrome and rarely pleural effusions In AV access hemodialysis patients specifically; engorged, pulsatile AVF, positive arm elevation test, increased difficulty needling access, increased bleeding post dialysis, poor dialysis adequacy Diagnosis High risk of suspicion should occur with patients with previous history of CVS, history of multiple catheters, physical features present Diagnostic imaging modalities should be used to confirm diagnosis including; duplex ultrasonography, angiography, magnetic resonance angiography 17
Vascular Access Education Initiative | 2015 CENTRAL VEIN STENOSIS Management of central vein stenosis Conservative management No intervention required asymptomatic patients require only close observation for any changes in symptoms Percutaneous transluminal angioplasty Treatment of choice for symptomatic central venous stenosis Can be performed alone or with stenting Initial success with angioplasty without stenting ranges between 70-90% Most patients require repeated angioplasty because lesions recur Resistant lesions or rapidly recurring lesions may have better resulst with cutting balloon or angioplasty plus stenting Surgery Due to potential for morbidity this should be considered only as last resort after repeated angioplasty with or without stenting has failed 18
Vascular Access Education Initiative | 2015 OTHER COMPLICATIONS Catheter-Associated Thrombus Catheter-Related Right Atrial Thrombus (CRAT) Difficult to Remove Embedded Catheter Serious complications include: pulmonary embolism, septic emboli, long-term central venous stenosis, cardiac arrhythmias Associated with an overall mortality rate of 18% Typically embedded or tethered inside the central vein system Thrombus <6 cm, recommend removal of the catheter and anticoagulation Options: open surgery, cutting and burying, endoluminal dilatation (see visuals slide 19) Treat with anticoagulation without removing catheter Thrombus >6 cm, cardiac abnormalities or contraindications to anticoagulation, consider surgical thrombectomy Duration of treatment depends on extent of thrombosis, risk of bleeding and ongoing need for use of catheter Burying the catheter has been associated with infection; however, a single-centre experience with endoluminal dilatation suggests this approach may result in uncomplicated removal of such catheters Consider catheter exchange over guidewire with tip in superior vena cava rather than right atrium or thrombolysis Although limited data and no general guidelines, anticoagulation for 3 mths is a general recommendation Note: Central Vein Stenosis can be found in Chapter 4 19
Vascular Access Education Initiative | 2015 BALLOON ASSISTED ENDOLUMINAL DILATATION (for removal of embedded catheters) Photos courtesy of Dr Adnan Hadziomerovic 20
Vascular Access Education Initiative | 2015 LAST OPTION ACCESS Commonly used last access options include: (for more detail see Chapter 3: Arteriovenous access) HeRO Device (Hemodialysis Reliable Outflow) When inserted, bypasses any central venous stenosis without the need for a graft-to-vein anastomosis (See Chapter 3) Translumbar Catheters Inserted into the inferior vena cava via the translumbar route Reserved for dialysis patients who have exhausted all other access options Technically challenging, and may be associated with procedure related complications (eg retroperitoneal hematoma) Transfemoral Catheters Less technically challenging to insert Consider catheter length (usually 70 cm in length; cuff at 45 cm) and infection prophylaxis, given their exit site in close proximity to the groin 21
Vascular Access Education Initiative | 2015 SUMMARY OF RECOMMENDATIONS Catheter dysfunction is a frequent and common cause of catheter loss; may occur early, most often the result of mechanical issues or late, most often due to thrombotic occlusion or fibrin sheath Sodium citrate (4%) or concentrated heparin solutions (1000 units/ml) are the current standard recommended anticoagulant locking solutions infused into the catheter lumens to maintain catheter patency between hemodialysis treatments Antiplatelet agent and systemic oral anticoagulation have not proven beneficial in improving catheter patency, and may increase risk of bleeding Thrombolytic agents can be used to successfully restore patency in thrombotic/occluded catheters. If unsuccessful, catheter exchange with fibrin sheath plasty is recommended Central vein stenosis is a common vascular access complication, occurring in up to 40% of hemodialysis patients with a catheter Central vein stenosis is often asymptomatic until creation of an ipsilateral arteriovenous access 22
Vascular Access Education Initiative | 2015 SUMMARY OF RECOMMENDATIONS Reduce risk factors for central vein stenosis: minimize number and exposure time to central venous catheters, CIEDs, PICCs. Attempt creation of arteriovenous access on opposite side of any central venous access device Symptomatic CVS should be treated with percutaneous transluminal angioplasty. Stenting is generally not recommended except for recoil elastic lesions and recurrence within 3 months of angioplasty. Surgery should be considered a last resort Right atrial thrombus is a less common, but serious complication of catheters, requiring systemic anticoagulation and possibly catheter removal In the event of poor arteriovenous access and/or loss of upper extremity central veins, alternative access options include transfemoral catheters, translumbar catheters, and the HeRO device. These options require skilled interventionalists, and optimal approaches are dictated by local experience and expertise Balloon-assisted endoluminal dilatation can be used for removal of embedded catheters 23