Otosclerosis in Adults: Causes and Symptoms
Otosclerosis is a common cause of progressive hearing loss in adults, affecting the otic capsule bone. Learn about its inheritance, prevalence, clinical presentation, and histopathology.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Otosclerosis By DR Abdulhussein Kareem
Otosclerosis is the most common cause of progressive conductive hearing loss in adults with prevalence grater in women than men,2;1 ratio. It is a disease of bone that is unique to the otic capsule. It can cause conductive ,SNHL or both . Hearing loss due to fixation of stapes was first described by Valsalva in 1704 after postmortem dissection of a deaf patient.
In 1841,Toynbee identified ankylosis of the stapes in a series of temporal bone specimens and concluded that this was a common cause of deafness. In 1893,Politzer referred to the bony fixation of stapes as otosclerosis. Siebenmann first revealed ,on histopathologic examination, that the lesion seemed to begin as spongification of the bone and termed the process otospongiosis.
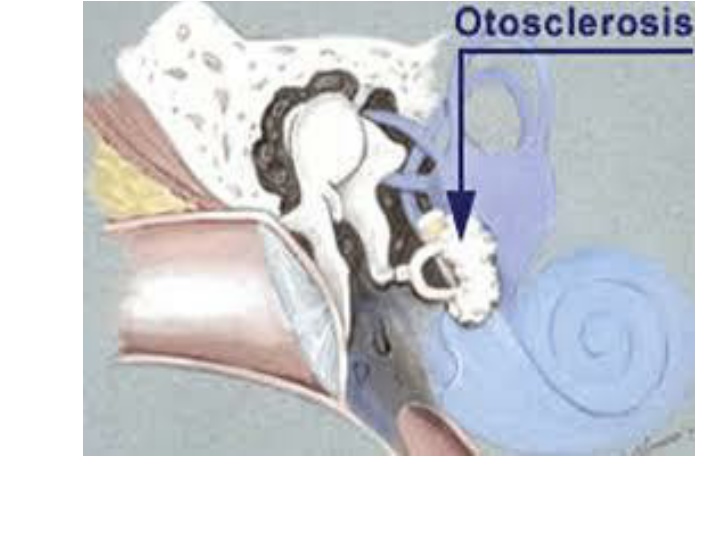
Clinically .the patients present with progressive hearing loss which is conductive if the lesion involves the stapes. Stapedial fixation most commonly begins at the anterior oval window along the fissula ante fenestram,the process may progress to involve the entire footplate or may continue anteriorly to involve the cochlea causing SNHL.
Otosclerosis is inherited as autosomal dominant disease with variable penetrance between25%and 40%. 60% of pt with clinical otosclerosis have a positive family history. Several studies have suggested a link between the measles virus and otosclerosis. The condition may be accelerated by hormonal changes during pregnancy.
It is more common in Caucasians with clinical prevalence of 0.3% to0.4% while histological otosclerosis is 10% to 12%. It is rare in Africans and Asians. Histopathology; Otosclerosis is a disorder of endochondral bone remodeling limited to the otic capsule . Bone is absorbed by osteoclasts and new bone is deposited by osteoblasts.
In the initial osteoclastic phase, there is resorption of lamellar otic capsule bone (otospongiotic ) active phase. Early lesions appear adjacent to the fissula ante fenestram near the anterior oval window. The extent and location of these lesions vary, some are small and do not involve the stapes. As the disease advances ,the lesions spread across the stapedial annular ligament and cause stapedial fixation.
If the lesion progresses medially to involve the endosteum of the cochlea,SNHL results. It may spread in both directions ,resulting in mixed hearing loss, occasionally the lesion may involve only the cochlea, causing an isolated SNHL.
Clinical evaluation; History; Hearing loss is typically of gradual onset and progresses slowly over several years. 75% of otosclerosis cases are bilateral and present at late teens or 20s,but may be delayed till the age of 30 or 40 years. The hearing loss is usually conductive and the pt reports that hearing is better in noisy environment(paracusis of Willis).
Unilateral hearing loss may be less noticeable to the pt, although there may be difficulty with determining the direction of sound. Tinnitus often accompanies otosclerosis and may be pulsatile or continuous. Pulsatile tinnitus occurs during the active phase due to increased vascularity of otospongiotic lesions. Continuous tinnitus is seen in cochlear otosclerosis and tends to persist. Both types will improve after surgery.
Two-thirds of pt with otosclerosis have family history of hearing loss. History of ear infections or trauma. Associated symptoms like autophony and or dizziness with loud sounds (superior canal dehiscence).
Physical examination; Careful otoscopic examination by otoscope, endoscope or microscope to rule out middle ear diseases, Use of Siegel s pneumatic apparatus to check the mobility of tympanic membrane and exclude small tympanic mem perforations. In the active phase there is red blush on the promontory(Schwartz sign).
Tuning fork examination; Rinne, Weber and Schwabach tests. Audiometry; The audiometric evaluation includes air conduction, bone conduction and speech audiometry done by a trained audiologists. The typical audiogram shows a unilateral or bilateral air-bone gap usually greater in the low-frequencies.
Bone conduction may show a distinct notch-like decrease at 2000Hz(Carhart notch).due to impedance mismatch of the cochlea from stapes fixation. Tympanometry ; The middle ear pressure is not affected by otosclerosis and the tympanogram is normal(A)or with slightly increased stiffness(As). Greater stiffness or shallower type As may indicate tympanosclerosis or other ossicular fixation.
Type Ad tympanogram may suggest ossicular discontinuity as a cause of cond HL. Acoustic reflexes are a sensitive measures of the movement of the stapes and the reflex is absent in otosclerosis ,in early stages ,the reflex may be abnormal (negative on-off effect or diphasic reflex. With more advanced disease, the reflex will be absent and even the contralateral side will be affected.
Radiology ; Otosclerosis diagnosis is based on history and audiometric findings,however,temporal bone CT scan can be useful in certain cases. On CT imaging, early stapedial otosclerosis can be confirmed by the presence of a lucency at the ant oval window while in cochlear otosclerosis, there is a ring-like lucency around the cochlea(halo sign).
These lucent lesions are due to demineralization of otic capsule bone (otospongiosis). In advanced lesions, the disease can be confirmed by the presence of increased density and marked thickening of sclerotic bone around the otic capsule.
Treatment; 1.Surgery 2.Hearing aids and other devices 3.Flouride therapy.
Surgery; John Shea performed the first stapedectomy in 1956 using teflon as a prosthesis. The outcome ,risk and complications should be discussed with the pt. Although the risk of SNHL is low, the pt should be informed about it and due to this possibility, the worst ear is selected for surgery
Stapedotomy technique; 1.Canal injections; Four quadrant canal block and vascular strip injection with1%lidocaine and 1:100,000 adrenaline. 2.Create tympanomeatal flap incisions and elevate flap, entering the middle ear beneath annulus and freeing corda tympani from adhesions under the tympanic membrane. 3.Remove bone from poster superior canal wall with curette or microdrill to see the facial nerve and pyramidal process.
4.Palpate ossicular chain to confirm stapes fixation. 5.Measure distance from lateral surface of incus to footplate. 6.Use laser to make opening in the centre of foot plate. 7.Use microdrill to weaken posterior crus and create fenestra. 8.Place piston prosthesis into fenestra and onto incus.
9.Crimp prosthesis hook. 10.Down fracture stapes superstructure and remove . 11.Place tissue graft around prosthesis to form seal. Surgery is usually performed under local anesthesia.
Postoperative care; The pt head is elevated 30 degrees to reduce the perilymph pressure in the vestibule for 30 to 40 minutes. Pt can be discharged next day . Next visit 1 week later. Avoid wt lifting. Sneezing and cough with open mouth.
Better to avoid diving for 3 weeks The first audiogram is done 3 months after surgery. Stapes prostheses; The choice of prosthesis depends on ease of use, device safety profile and long-term stability of hearing outcome. Piston prostheses are most commonly used.
These prostheses contain a teflon piston with a wire loop fashioned from stainless steel, titanium or platinum wire. Recently .heat-activated memory-shape prostheses were developed. It contains nitinol which is a metal alloy of nickel and titanium that can conform to a predetermined shape with heat activation. Once positioned on the incus, a laser, bipolar or heating filament can be used to self-crimp the prosthesis.
Postoperative complications; 1.SNHL, occurs in less than 1% of cases and the cause is unclear. 2.Vertigo,mild vertigo or dizziness is common and occurs in 5% of cases ,lasts for few days but if becomes severe and prolonged ,PTA should be done urgently to exclude complications.
3.Facial paralysis, rarely occurs ,incomplete and responds quickly to steroids. It may be due to viral reactivation. 4.Tinnitus,after stapedectomy, most pt note an improvement in tinnitus but few pt may develop new-onset tinnitus.it may be due to serous labyrnthitis and may improve as the ear continue to heal. 5.Hyperacusis ,most pt complain of some degree of phonophobia which will resolve gradually.
6.Taste disturbance, occurs in one-third in the form of temporary dry mouth, tongue soreness or a metallic taste usually subsides in 3 to 4 months. 7.Perilymph fistula, mostly seen after stapedectomy and gelfoam patch but it is less with the use of small fenestra technique. Pt complain of mixed hearing loss ,unsteadiness and rarely vertigo Treated by removal of prosthesis, placement of a tissue graft over the oval window, and replacement with another prosthesis.
Hearing aids; All pt with CHL ,caused by otosclerosis may use hearing aids as an alternative to surgery. If the pt has a significant SNHL ,a hearing aids may be required even after successful stapedectomy. Many pt with advanced otosclerosis require time to adjust to the new hearing level and are sensitive to the sound of their hearing aid.
It may take 4 months before these pt can tolerate and benefit from the hearing aid. Fluoride therapy; This therapy has been shown to reduce the progression of SNHL. The mechanism of action is by conversion of the active otospongiotic lesion to more stable otosclerotic lesion.
Dose ;8 mg three times daily until hearing loss stabilizes. Gastric distress is the most common SE. Recently bisphosphonates(risedronate and zoledronate) are more effective in decreasing the progression of SNHL with otosclerosis .
For far advanced otosclerosis with progression to profound hearing loss with significant deterioration in speech discrimination despite the use of a hearing aid ,pt are considered for cochlear implant. Endolymphatic hydrops may occur with otosclerosis as 2 separate disease entities or as a result of otosclerosis. Stapedectomy in the presence of uncontrolled Meniere's disease can result in dead ear and should be avoided.
In such pt fluoride therapy and hearing aids are acceptable treatment.