Pediatric Surgery 2018: Understanding Neonatal Intestinal Obstruction
Explore the field of pediatric surgery and its differences from general surgery, focusing on neonatal intestinal obstruction. Learn about atresia, malrotation of midgut, and treatment approaches. Delve into the embryology of malrotation, its presentation, and diagnostic considerations for infants. Enhance your understanding of pediatric surgery concepts through a comprehensive overview provided by Dr. Ali E. Joda.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
PEDIATRIC SURGERY-2018 No. :3 Attendance: Obligatory Type of lecture: theory Place : Hall no.4 college of medicine Mustansiriyah University . Date : Monday 5th of March 2018. Time : 8:00 9:00 AM. Students: 4th year / college of medicine / Mustansiriyah University By : Dr. Ali E. Joda M.B.Ch.B. - F.I.C.M.S. - pediatric surgeon. E. mail : ali.egab.joda@uomustansiriyah.edu.iq
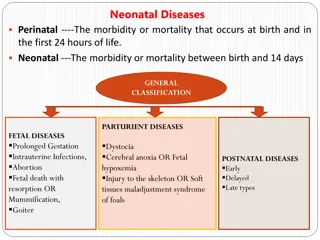
Objectives:- What is the field of pediatric surgery & how it differs from general surgery? By the end of this lecture, you have to be able to recognize the main features of neonatal intestinal obstruction & how you can approach to infant with this problem. What is atresia & where it could be occur in gastrointestinal tract? How can you differentiate it from other causes of intestinal obstruction like malrotation of midgut & meconium ileus. What are the main lines of treatment?
Malrotation of midgut Embryology :- The intestinal tract is first recognized at 4 weeks of gestation & divided into foregut , midgut , & hindgut. During the next few weeks ; growth & development of midgut is faster than that of abdominal cavity , so the midgut normally herniated out of the peritoneal cavity into the umbilical cord then returns to abdominal cavity at 10 weeks of gestation. The return of intestine accompanied by a process of rotation & fixation, the axis of rotation is superior mesenteric artery (SMA).
The proximal limb of midgut (duodenojejunal junction) is fixed in the upper left quadrant of the abdomen while the distal limb of midgut (cecocolic ) is fixed in the right lower quadrant of the abdomen. The normal rotation of midgut is critical for the formation of broad base mesentery with its fixation to the posterior body wall. Any error of normal rotation & fixation will lead to formation of narrow midgut mesentery & lack of fixation to the posterior body wall , which allows axial rotation of midgut around SMA resulting in midgut volvulus.
Normal malrotation malrotation with volvulus
Presentation :- The presentation is age dependent : (1) midgut volvulus (top emergency). (2) partial duodenal obstruction (recurrent intestinal obstruction). (3) chronic non- specific abdominal complaints.(4) asymptomatic: discovered accidentally during investigation or during surgery for other reason. The classic & most common presentation is volvulus of midgut in neonatal period in form of acute onset of bilious vomiting in a previously healthy infant , mild or just upper abdominal distention (secondary to duodenal obstruction) , dehydration , abdominal wall erythema , peritonitis. Hematemesis , malena may result from intestinal mucosal ischemia.
partial duodenal obstruction may result from (1)kinking of abnormally positioned duodenum , (2)narrowing of duodenal lumen by torsion of partial volvulus , (3)extrinsic obstruction by Ladd's band ( peritoneal band from cecum to posterior abdominal wall crossing the duodenum) , (4)associated intrinsic duodenal atresia.
Diagnosis :- Midgut volvulus is true surgical emergency because the delay in diagnosis or operative correction will lead to necrosis of the whole midgut & death. Plain abdominal X-ray : distended stomach & proximal duodenum with little air in distal small bowel , double bubble sign , or dilated loops of bowel with multiple air-fluid levels. Upper GI contrast study (barium meal) give us the definitive diagnosis : complete obstruction of second or third part of duodenum , corkscrew (coiled spring ) appearance of duodenum & jejunum , position of DJ is to the right of midline (normally it is to the left of midline).
Barium meal volvulus of mid-gut de-torsion of volvulus
Treatment :- Immediate resuscitation , IVF , NG tube , Foley's catheter , broad spectrum antibiotics , prepare blood , then laparotomy (Ladd's procedure):- 1. Detorsion in counterclockwise direction. 2. Division of Ladd's band. 3. widening of the mesenteric base. 4. Incidental appendicectomy. 5. Redistribution of bowel (small in the left side, large in the right side).



 is")