Protein Synthesis Inhibitors I)
This content by Hala Aqeel Shams delves into the topic of Protein Synthesis Inhibitors. It covers various aspects of inhibiting protein synthesis and its implications in the field of clinical pharmacology. The author's detailed exploration provides valuable insights for those studying or working in this area, offering a comprehensive resource on the subject.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Protein Synthesis Inhibitors I) ) By Hala Aqeel Shams M.B.Ch.B/MSc. Clinical pharmacology
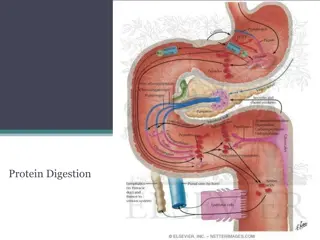
Protein synthesis inhibitors exert their antimicrobial effects by targeting bacterial ribosomes and inhibiting bacterial protein synthesis. Most of these agents exhibit bacteriostatic activity. Bacterial ribosomes differ structurally from mammalian cytoplasmic ribosomes and are composed of 30S and 50S subunits (mammalian ribosomes have 40S and 60S subunits)
Sites of drug action: The basic steps in bacterial protein synthesis include the binding of aminoacyl transfer RNA (tRNA) to the ribosome formation of a peptide bond translocation. Each type of antibiotic acts at a specific site on the ribosome to inhibit one or more steps in protein synthesis. Tetracyclines and aminoglycosides act at the 30S ribosomal subunit. Macrolides, chloramphenicol, quinupristin/dalfopristin, and clindamycin act at the 50S ribosomal subunit.
Tetracyclines competitively block binding of tRNAto the 30S subunit and thereby prevent the addition of new amino acids to the growing peptide chain. The reversibility of this effect accounts for the bacteriostatic action of tetracyclines. Aminoglycosides also bind to the 30S subunit, where they interfere with the initiation of protein synthesis and cause misreading of the genetic code so that the wrong amino acid is inserted into the protein structure. These irreversible actions account for the bactericidal effects of these antibiotics.
Macrolides, chloramphenicol, and quinupristin/dalfopristin block peptidyl transferase, the enzyme that catalyzes the formation of a peptide bond between the latest amino acid and the nascent peptide. Macrolides and clindamycin prevent translocation of the nascent peptide from the acceptor or aminoacyl site (A site) to the peptidyl site (P site) on the ribosome, which in turn prevents binding of the next aminoacyl tRNAto the ribosome.
1. TETRACYCLINES Tetracyclines originated from actinomycetes soil bacteria. Tetracyclines enter susceptible organisms via passive diffusion and by an energy-dependent transport protein mechanism unique to the bacterial inner cytoplasmic membrane. Tetracyclines concentrate intracellularly in susceptible organisms.
Tetracyclines bind reversibly to the 30S subunit of the bacterial ribosome prevents binding of tRNAto the mRNA ribosome complex inhibiting bacterial protein synthesis(bacteriostatic)
Antibacterial spectrum bacteriostatic antibiotics broad spectrum antibiotics: effective against gram-positive and gram-negative bacteria, protozoa, spirochetes, mycobacteria, and atypical species. they are commonly used for the treatment of Chlamydia infections and moderately severe acne. these antibiotics suppress the growth of Propionibacterium acnes, an organism found on the skin that can infect sebaceous glands.
Doxycycline and minocycline have also been used to treat skin and soft tissue infections caused by methicillin- resistant Staphylococcus aureus (MRSA). Tetracyclines are also used in the treatment of brucellosis, ehrlichiosis, and granuloma inguinale.
Resistance Efflux pump that expels drug out of the cell, thus preventing intracellular accumulation. Enzymatic inactivation: production of bacterial proteins that prevent tetracyclines from binding to the ribosome. The practice of including tetracyclines in animal feeds to promote weight gain has contributed to the development and transmission of tetracycline resistance around the world. Note: resistance to one tetracycline does not confer universal resistance to all tetracyclines, and the development of cross-resistance may be dependent on the mechanism of resistance. 1. 2. 3.
Pharmacokinetics Absorption: adequately absorbed after oral ingestion. administration with dairy products or other substances that contain divalent and trivalent cations (for example, Mg, Ca, aluminum antacids, iron supplements) decreases absorption, particularly for tetracycline and omadacycline, due to the formation of nonabsorbable chelates. doxycycline , minocycline and omadacycline are available as oral and intravenous (IV) preparations 1.
2. Distribution: Penetrate into most body fluids and concentrate well in the bile, liver, kidney, gingival fluid, and skin. they bind to tissues undergoing calcification (for example, teeth and bones) or to tumors that have high calcium content. Poor penetration to BBB except minocycline and doxycycline achieve therapeutic levels in the cerebrospinal fluid (CSF). Minocycline also achieves high concentrations in saliva and tears, rendering it useful in eradicating the meningococcal carrier state. All tetracyclines cross the placental barrier and concentrate in fetal bones and dentition. 3. Elimination: All excreted unchanged in the urine Minocycline and Doxycycline undergoes hepatic metabolism and eliminated via the bile into the feces. Doxycycline is preferred in patients with renal dysfunction,
Adverse effects 1. GIT distress : results from irritation of the gastric mucosa may be minimized through co-administration with food (other than dairy products) or fluids and the use of capsules rather than tablets. [Note: Tetracycline and omadacycline should be taken on an empty stomach.] 2. Hepatotoxicity: high doses pregnant women preexisting hepatic dysfunction or renal impairment 1. 2. 3.
3. Effects on calcified tissues: Deposition in the bone and primary dentition occurs during the calcification process in growing children. This may cause discoloration and hypoplasia of teeth (yellow-brown or gray mottling of a significant portion of the enamel of the front teeth can be seen) and a temporary stunting of growth. For this reason, the use of tetracyclines is limited in pediatrics.
4. Phototoxicity: Severe sunburn may occur in patients receiving a tetracycline who are exposed to sun or ultraviolet rays. This reaction results from the absorption of ultraviolet radiation by the tetracycline after its accumulation in the skin. This toxicity is encountered with any tetracycline, but more frequently with tetracycline and demeclocycline. Patients should be advised to wear adequate sun protection.
5. Other effects: Benign, intracranial hypertension (pseudotumor cerebri) characterized by headache and blurred vision may occur rarely in adults. Although discontinuation of the drug reverses this condition, it is not clear whether permanent sequelae may occur. Vestibular dysfunction manifested as dizziness, vertigo, and tinnitus may occur, particularly with minocycline. Contraindications: pregnant or breastfeeding women in children less than 8 years of age. 1. 2.
2. GLYCYLCYCLINES Tigecycline ,a derivative of minocycline, is the first member of the glycylcycline antimicrobial class. It is indicated for: complicated skin and soft-tissue infections complicated intra- abdominal infections community-acquired pneumonia. 1. 2. 3. Mechanism of action bacteriostatic Reversible binding to the 30S ribosomal subunit and inhibiting bacterial protein synthesis.
Antibacterial spectrum broad-spectrum including: methicillin- resistant staphylococci (MRSA), multidrug- resistant streptococci, vancomycin-resistant enterococci (VRE), extended-spectrum -lactamase producing gram- negative bacteria, Acinetobacter baumannii, and many anaerobic organisms. Tigecycline is not active against Morganella, Proteus, Providencia, or Pseudomonas species. Resistance Tigecycline was developed to overcome the emergence of tetracycline class resistant organisms Resistance to tigecycline has been observed and is primarily attributed to overexpression of efflux pumps.
Pharmacokinetics Following IV infusion, tigecycline exhibits a large volume of distribution. It penetrates tissues well but achieves low plasma concen- trations. Consequently, tigecycline is a poor option for bloodstream infections. the primary route of elimination is biliary/fecal. dose adjustments is recommended in hepatic dysfunction. No dosage adjustments are necessary for patients with renal impairment
Adverse effects Nausea, vomiting, acute pancreatitis Elevations in liver enzymes and serum creatinine may also occur. Other adverse effects are similar to those of the tetracyclines and include photosensitivity, pseudotumor cerebri, discoloration of permanent teeth when used during tooth development, and fetal harm when administered in pregnancy. Tigecycline may decrease the clearance of warfarin. Therefore, INR should be monitored closely when it is co- administered with warfarin. 1. 2. 3. 4.
3. Aminoglycosides (amikacin ,gentamicin , tobramycin and streptomycin) highly water-soluble compounds originally isolated from soil actinomycetes used for the treatment of infections due to aerobic gram- negative bacilli. If the compounds are isolated from Streptomyces, they are named with the suffix mycin and if they are from Micromonospora, the compounds would be having the suffix micin.
Mechanism of action they are bactericidal they bind irreversibly to 30S ribosomal subunit, where they interfere with the ribosomal apparatus and cause the 30S subunit of the completed ribosome to misread the genetic code. They are ineffective with anaerobic infections as they depend on an oxygen-dependent system that transports the drug across the cytoplasmic membrane of susceptible organism
They have concentration-dependent activity: their efficacy is dependent on the maximum concentration (Cmax) of the drug above the minimum inhibitory concentration (MIC) of the organism. For aminoglycosides, the target Cmax is 8 to 10 times the MIC. They also exhibit a post-antibiotic effect (PAE): which is continued bacterial suppression after drug concentrations fall below the MIC. The larger the dose, the longer the PAE. Because of these properties, high-dose extended-interval dosing is commonly utilized. This dosing strategy also reduces the risk of nephrotoxicity and increases convenience.
Antibacterial spectrum The aminoglycosides are effective for the majority of aerobic gram-negative bacilli, such as Pseudomonas aeruginosa, Klebsiella pneumoniae, and Enterobacter sp. aminoglycosides are often combined with a -lactam antibiotic to employ a synergistic effect, particularly in the treatment of Enterococcus faecalis and Enterococcus faecium infective endocarditis.
Resistance inactivation of the drugs by bacterial enzymes that combine the drugs with acetate, phosphate, or adenylate. Each of these enzymes has its own aminoglycoside specificity; therefore, cross-resistance cannot be presumed. [Note: Amikacin is less vulnerable to these enzymes than other antibiotics in this group.] decreased binding of the drugs to the 30S ribosomal subunit or to decreased uptake of the drugs by porins in bacterial membranes and also efflux pumps.
Pharmacokinetics Absorption: Poor oral absorption because: highly polar and polycationic structure therefore, all aminoglycosides (except neomycin) must be given parenterally to achieve adequate serum concentrations. 1. Note: Neomycin is not given parenterally due to severe nephrotoxicity. It is administered topically for skin infections or orally to decontaminate the gastrointestinal tract prior to colorectal surgery.
2. Distribution: due to their hydrophilicity and penetration into most body fluids is variable. Poor concentrations in CSF, even in the presence of inflamed meninges, so intrathecal or intraventricular routes may be utilized in CNS infections. All aminoglycosides cross the placental barrier and may accumulate in fetal plasma and amniotic fluid. 3. Elimination: More than 90% of the are excreted unchanged in the urine. dose adjustments are required in patients with renal dysfunction Neomycin is primarily excreted unchanged in the feces. poor tissue concentrations
Adverse effects 1. Ototoxicity: Ototoxicity (vestibular and auditory) is directly related to high plasma concentrations and the duration of treatment. Aminoglycosides accumulate in the endolymph and perilymph of the inner ear. Patients receiving concomitant ototoxic drugs, such as cisplatin or loop diuretics, are particularly at risk. Vertigo (especially in patients receiving streptomycin). cross the placenta fetal ototoxicity contraindicated during pregnancy(deafness may be irreversible)
2. Nephrotoxicity: one of the most common causes of drug-induced renal failure. When the drugs accumulate in proximal tubule cells, disrupting calcium-mediated transport processes This results in kidney damage ranging from mild, reversible renal impairment to severe irreversible acute tubular necrosis. they may also cause glomerular toxicity.
3. Neuromuscular paralysis: This adverse effect is associated with(high doses infused over a short period) or concurrent administration with neuromuscular blockers. Patients with myasthenia gravis are particularly at risk. Prompt administration of calcium gluconate or neostigmine can reverse the block that causes neuromuscular paralysis. 4. Allergic reactions: Contact dermatitis is a common reaction to topically applied neomycin