Proteinuria is the presence of excess proteins in the urine, typically kept in check by the glomerulus and tubules. Learn about normal protein excretion levels and the intricate processes involved in renal handling of proteins.
Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
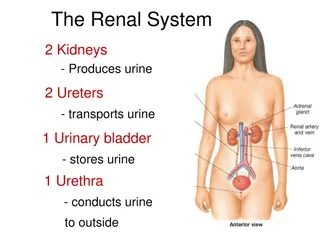
PROTEINURIA By Mohamad A. Sobh, MD, FACP Prof. & Head of Nephrology Urology & Nephrology Center Mansoura University Egypt
Plasma Protein Delivery to the Nephrons Protein conc. in plasma Renal plasma flow X 1440 (min/day) Protein delivery / day = ~70 g/L = 625 ml/min = ~900 L/day = 63000 g/day = 63 kg/day Renal Handling of Proteins Despite the delivery of many grams of plasma proteins to the nephrons each day , protein is normally present in only small quantities in the urine due to: 1-The glomerulus restricts the filtration of proteins 2-The tubules reabsorb most of the filtered proteins Glomerular Restriction of Proteinuia Glomerular capillaries are highly efficient sieving filter: Free water 150-180 L/day + electrolytes & other solutes (<10 000 Daltons) are freely filtered . Retain the permeation of macromolecules of the size or greater than albumin (cut-off 1.5 nm) on the basis of size, charge, shape and deformability .
Filtration Barrier 1- Endothelial cell fenestra (1000A) 2- -ve charged BM: type IV collagen network filled with polyanionic heparan sulphate proteoglycans 3- -ve charged epithelial cells with foot prcesses (200-300A in between) covered by slit diaphragm with openings 4x14 nm However, hemodynamic factors also play a role in glomerular handling of macromolecules Tubular Reabsorption 500-1000 mg of albumin is filtered by the glomeruli each day yet only 30 mg/day reaches the final urine, the balance being absorbed by the proximal tubules Many low-molecular weight proteins and peptides are freely filtered by the glomerulus and are similarly reabsorbed & degraded by the renal tubules; e.g. lysozymes, ribonuclease, light chains, B2 microglobulin, insulin, GH, & PTH
Normal Urinary Protein Excretion Normally, urinary protein excretion is <150 mg/day in adults & <140 mg/m2/day in children It is usually not detected by ordinary methods It is composed of : o Mucoproteins (Tamm-Horsfall glycoprotein): 70 mg o Blood group related substances: 35 mg o Albumin : <30 mg o Immunoglobulin: 6 mg o Mucopolysaccharides : 16 mg o Other ptns e.g. hormones & enzymes: v. small amounts
Measurement of Proteinuria Qualitative techniques: Precipitation techniques: Heating, or adding glacial acetic acid, , trichloroacetic acid or sulfosalicylic acid (SSA, the most popular) Turbidity may be graded by comparing to (urine + water): trace=20mg/dl, 4+=1g/dl or measured by turbidometry It detects both albumin, globulin and BJ proteins +Ve precipitation with negative dipstick in globulinuria or BJ proteinuria Dipstick: Tetrabromophenolphthalein , induce a color change with protein . sensitive to albumin more than other proteins as globulin and mucoproteins and fails to detect bence jones proteinuria Trace: <30, 1+:>30, 2+: >100, 3+: >500 mg/dl False +ve: high SG, alkaline urine, UTI, antiseptics Quantitative techniques: - Total 24-hour urinary protein - Urinary protein/creatinine (U Pr/Cr) ratio (mg/mg or g/g) Urinary albumin/creatinine ratio is more accurate, especially in low-range proteinuria (<500 mg/d) but more expensive and less practical
Proteinuria is a secretion of an abnormal amount of protein in urine. Normal protein excretion per 24 hours in adults is less than 150 mg. Most of this protein is albumin and Tamm Horsfall protein with smaller amounts of immunoglobulins. False positive proteinuria by dip stick occurs mainly when urine is alkaline and very concentrated; or if the stick test is left in urine for long time. False negative proteinuria is observed when protein excretion is mainly Bence Jones proteinuria and when urine is very diluted. Bence Jones protein which is the light chain fraction of immunoglobulin appears in abnormal amounts in urine in cases of multiple myeloma, clots at temperature 45-55 C, above and below that range it dissolves in urine. Presence of Bence Jones proteinuria should be confirmed by immunoelectrophoresis. The causes of Bence Jone's proteinuria include: multiple myeloma, amyloidosis, adult Fanconi syndrome, benign monoclonal gammopathy and hyperparathyroidism.
Is a secretion in urine of ammount of albumin that is more than the physiologic one (>3o mg/d), but less than the detection lemit of the clinical depsick test. When first discovered was used as early marker for diabetic nephropathy, but now it is considered also as marker of endothelial cell injury. It is measured by RIA , ELISA ,and recently by special depstick test.
Selectivity of Proteinuria This test is done to evaluate the degree of damage in the GBM through comparing the amount of a large mol. Wt. protein in urine to that of another small mol. Wt. protein. If the damage is little, most of the filtered proteins will be of small mol. Wt. , while if the damage is large both large and small protein will pass easy. This is done by comparing the clearance of IgG to that of transferrin: CIgG/Ctransferrin . A value < 0.1 is selective while > 0.2 is non selective. Selective proteinuria is usually seen in MCN while non selective is seen in lesions as MCGN. Test for selectivity was introduced to avoid doing kidney biopsy. This can be considered sometimes when biopsy is risky but can not be generalized.
Orthostatic (Postural) Proteinuria Proteinuria present in the upright position only that disappears with recumbent position. Mostly below 2g/day occasionally heavier Seen in90% of young men presenting with isolated proteinuria Entirely benign, transient in 80% Persistent Isolated Proteinuria Isolated proteinuria persistent in all samples tested in both recumbent and upright states Seen in 5-10% of isolated proteinuria in healthy men Almost always a sign of structure renal disease with some risk of progression although prognosis is not bad in all cases Assessment will show a wide variety of renal lesions; e.g. GN Functional Proteinuria Proteinuria in association with high fever, strenuous exercise, exposure to cold, emotional stress, congestive heart failure, and other acute medical diseases This proteinuria disappears as soon as the precipitating factors has resolved It is glomerular in type due to changes in renal hemodynamics No progressive renal disease
Mechanism of proteinuria There are four known mechanisms for proteinuria: 1. Abnormality in permeability of the glomerular basement membrane because of glomerular disease or abnormal glomerular hemodynamics , usually albumen ( glomerular ) 2. Increased concentration of small molecular weight protein in blood (MW 60000- 70000) e.g. hemoglobin, myoglobin and immunoglobulin light chains. These will pass easily through the normal GBM ( overflow ) 3. Tubular disease with inadequate reabsorption of normally filtered proteins of MW <60000 e.g. B2-microglobulin ( tubular ). 4. Secretion by renal tubular cells of Tamm-Horsfall protein (urinary glycoprotein) ( secretory ).
Causes ( D.D) of Proteinuria I. Functional proteinuria: There is no organic change in the kidney tissue: it is usually less than 1 gm/d and is reversible. Possibly, it is due to hemodynamic changes or to minor glomerular disease which are reversible. a. Strenuous exercise b. Fever c. Orthostatic proteinuria d. Miscellaneous (Thyrotoxicosis, severe anaemia, CNS lesions) II. Tubular Proteinuria : Patients with proteinuria of 0.5-3.5 gm/d , Usually caused by tubular or tubulointerstitial diseases a. Acute interstitial nephritis. b. Chronic interstitial nephritis such as bacterial (pyelonephritis), gouty nephropathy , analgesic nephropathy or nephrolithiasis. c. Tubular diseases such as Fanconi syndrome, heavy metal intoxication (lead, cadmium), multiple myeloma, hypokalaemic nephropathy, polycystic kidney disease and medullary cystic kidney disease.
III.Glomerular Proteiuria : Usually caused by glomerular disease. A. Primary glomerular disease: Minimal change disease Membranous glomerulonephritis Focal-segmental glomerulonephritis Immunoglobulin A nephropathy Membranoproliferative glomerulonephritis B. Secondary glomerular disease: Acute poststreptococcal glomerulonephritis Collagen vascular diseases, HUS, TTP Metabolic diseases: DM, Amyloidosis, etc. Malignancy-associated Drugs (gold, nonsteroidal anti-inflammatory drugs, heroin, penicillamine) Infections (human immunodeficiency virus; hepatitis A, B, C) Obesity Reflux nephropathy Patients with proteinuria of more than 3.5 gm/d
Symptoms & Signs of Proteinuria Usually detected initially on routine urinalysis as an unexpected finding Patients may be completely asymptomatic Or may have many symptoms according to the magnitude of the proteinuria and/or the level of renal function: Foamy or frothy urine Varying grades of edema Nephrotic syndrome: proteinuria >3.5 grams/day classically presents with edema, hypoalbuminemia, and hypercholesterolemia Patients with glomerulonephritis may be asymptomatic or have hematuria, edema of new onset, pulmonary symptoms, hypertension and/or azotemia
Complications of Proteinuria Hypoalbuminemia Edema Increased hepatic lipoprotein synthesis Increased platelet aggregability Increased tubular protein reabsorption Possible tubular dysfunction Tubular damage Loss of proteins carrying vitamins, hormones and minerals Trace mineral deficiencies Vitamin D deficiency Hypocalcemia Loss of immunoglobulins Reduced cellular immunity Increased susceptibility to infection Athersclerosis, CAD, & CVD Alterations in coagulation factors Spontaneous thromboembolism Renal vein thrombosis Negative nitrogen balance Malnutrition Alteration in drug metabolism
Proteinuria and Progression of CKD 1-Persistently increased protein excretion is usually a marker of kidney damage 2-Proteinuria is a good predictor of progressive CRF 3-The rate of decline of renal function is proportional to the severity of proteinuria 4-Proteinuria may cause tubular atrophy and intrstitial fibroses. 5-Transudation of protein and proteinaceous material glomerular cells proliferation and increase synthesis of extracellular matrix (ECM) components glomeruloscleroses.
Investigations of a case of proteinuria 1.Characterization of proteinuria: After diagnosis of proteinuria by dip stick test, it should be confirmed by quantitative estimation of 24 hours proteinuria. Further assessment may include electrophoresis or immunoelectrophoresis to determine the type of abnormal protein excreted. 2.Urine analysis: For pus cells (to diagnose U.T. infection), RBCs and casts (to diagnose glomerular disease), also urine volume (oliguria or polyuria), pH of urine, specific gravity and test for glucosuria; and aminoaciduria and B2 microglobulin (may help in the diagnosis of tubular disease). 3. Blood and serologic examination: A. Kidney function tests: serum creatinine, creatinine clearance, electrolytes (Na, K, Ca, Po4). B. Total protein, albumin, cholesterol to diagnose nephrotic syndrome. C. Serologic examination e.g. for anti-DNA and complement component C3 and C4 for diagnosis of lupus erythematosus.
4.Radiologic assessment including: a.Examination of the kidney for its size, state of parenchyma, the presence of stone, back pressure change or pyelonephritic changes. It is achieved through ultrasound examination, plain X-ray, and CT. b. Investigations to discover malignancy which could be the etiologic cause of proteinuria e.g. skeletal survey for multiple myeloma, X-ray chest and bronchogram or CT scan for bronchogenic carcinoma. 5. Renal biopsy will give the final answer for the diagnosis of the kidney lesion causing proteinuria.













 Proteinuria")

 of Proteinuria")