Restless Leg Syndrome: Symptoms, Diagnosis, and Treatment
Restless Leg Syndrome (RLS) is a sensory-motor neurological disorder that affects individuals of all ages, with symptoms such as periodic limb movement and sleep disturbances. Learn about the types of RLS, diagnostic criteria, prevalence rates, and possible genetic influences. Early diagnosis and proper management can significantly improve quality of life for those affected by RLS.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Restless Leg Syndrome BY MBBSPPT.COM
Restless Leg Syndrome The first description of RLS is attributed to Thomas Willis in 1685. Ekbom coined the term restless legs. In 1945, Ekbom gave a full description of the syndrome based on a large series of patients. This condition is sometimes referred to as Ekbom's syndrome. MBBSPPT.COM 2
Restless Leg Syndrome Periodic limb movement (PLM) and Restless leg syndrome (RLS) are types of sleep disorders. While RLS is a clinical diagnosis, the diagnosis of PLM is made by polysomnography. They share the same pathophysiology and often respond to the same treatment. The epidemiological studies have reported the prevalence between 2% and 15%. Rangarajan et al. (2007) found a prevalence of 2% from the door-to-door survey in Bangalore, India. MBBSPPT.COM 3
Restless Leg Syndrome RLS is a lifelong sensory-motor neurological disorder that often begins at a very young age but is mostly diagnosed in the middle or later years. Prevalence of RLS increases with age. MBBSPPT.COM 4
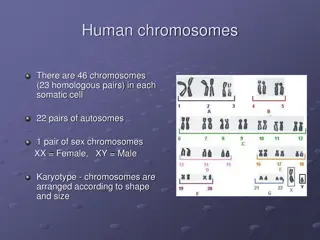
Restless Leg Syndrome The prevalence is greater in women than in men, and the disease is gradually progressing. Family studies of RLS suggest an increased incidence ( 40%-50%) in first-degree relatives of idiopathic cases. Autosomal dominant mode of inheritance (Hening et al., 2009). Linkage analysis documented significant linkage to at least six different chromosomes (12q, 14q, 9p, 2q, and 20p). MBBSPPT.COM 5
Types of RLS There are two types of RLS: 1. Early onset: Age of onset is less than 45 years, tends to cluster in families and progresses slowly with a female to male ratio of 2:1. 2. Late-onset: Age of onset over 45, has an equal male to female ratio, more rapid progression, more severe and more frequent symptoms, no familial clustering and are more commonly associated with radiculopathy, neuropathy or myelopathy. MBBSPPT.COM 6
Diagnostic Criteria The diagnosis rests entirely on clinical features and is based on the International Restless Legs Syndrome Study Group (IRLSSG) criteria first established in 1995 (Walters, 1995) and modified slightly in 2003 (Allen et al., 2003). These criteria include essential, supportive, and associated features. All four essential diagnostic criteria are needed for establishing the diagnosis. MBBSPPT.COM 7
Clinical Diagnostic Criteria for Idiopathic Restless Legs Syndrome Essential Criteria An urge to move the legs, usually accompanied by or caused by uncomfortable sensations in the legs. The urge to move or unpleasant sensations beginning or worsening during periods of rest or inactivity, such as lying or sitting. The urge to move or unpleasant sensations are partially or totally relieved by movement such as walking or stretching, at least as long as the activity continues. The urge to move or unpleasant sensations are worse in the evening or night than during the day or only occur in the evening or night. MBBSPPT.COM 8
Clinical Diagnostic Criteria for Idiopathic Restless Legs Syndrome Supportive Features Dopaminergic responsiveness Presence of periodic limb movements in sleep or wakefulness Positive family history Associated Features Usually progressive clinical course Normal neurological examination in the idiopathic form Sleep disturbance MBBSPPT.COM 9
Symptoms The sensory manifestations of RLS include intense disagreeable feelings described as creeping, crawling, tingling, burning, aching, cramping, knifelike, or itching sensations. These creeping sensations occur mostly between the knees and ankles. Sometimes, similar symptoms occur in the arms or other parts of the body, particularly in advanced stages of the disease. Approximately 15% to 20% of patients complain of actual pain. MBBSPPT.COM 10
Symptoms Most of the movements, particularly in the early stages, are noted in the evening while the patients are resting in bed. In severe cases, however, movements may be noted in the daytime while subjects are sitting or lying down. At least 80% of RLS patients have PLMS, and many also have periodic limb movements in wakefulness. MBBSPPT.COM 11
Secondary RLS The term secondary RLS is used whenever this condition is found in association with another medical condition. The most frequently found associations are renal failure, iron deficiency and pregnancy. RLS can be associated with pregnancy typically after 20th week and the incidence is estimated to be around 20%. RLS in association with hemodialysis population is estimated to be around 20% and the disease is usually more severe than primary RLS. Lower levels of ferritin have been noted in patients with RLS in comparison with controls. MBBSPPT.COM 12
Causes of Symptomatic or Comorbid Restless Legs Syndrome Medical Disorders Neurological Disorders Anemia: iron and folate deficiency Polyneuropathies Diabetes mellitus Amyloidosis Lumbosacral radiculopathies Uremia Amyotrophic lateral sclerosis Gastrectomy Cancer Myelopathies Chronic obstructive pulmonary disease Peripheral vascular (arterial or venous) disorder Multiple sclerosis Rheumatoid arthritis Parkinson disease Hypothyroidism Drugs and Chemicals Poliomyelitis Caffeine Neuroleptics Isaacs syndrome Withdrawal from sedatives or narcotics Hyperekplexia (startle disease) Lithium, nifedipine MBBSPPT.COM 13
Conditions That Mimic Restless Legs Syndrome Presenting with Nocturnal Leg Discomfort Presenting with Excess Restlessness Small-fiber neuropathies Akathisia Claudication Degenerative disease Venous stasis/varicose veins Disorders of abnormal muscular activity Myalgias Myokymia Arthritis Hypnic jerks Radiculopathies Essential myoclonus Presenting with Unusual Motor Activity Combined with Leg Discomfort Orthostatic tremor Anxiety/depression Painful muscle cramps including nocturnal leg cramps Periodic limb movement disorder Syndrome of painful legs and moving toes Restlessness due to orthostatic hypotension Causalgia-dystonia syndrome Attention-deficit hyperactivity disorder Muscular pain-fasciculation syndrome MBBSPPT.COM 14
Pathophysiology The pathophysiology and the site of CNS dysfunction in idiopathic or primary RLS remains unclear. Abnormalities in the body s use and storage of iron and dopamine dysfunction, which could involve changes in dopamine receptors or dopamine uptake . Iron is a necessary cofactor for tyrosine hydroxylase, the rate-limiting enzyme in dopamine synthesis, and iron deficiency may decrease the number of dopamine D2 receptor binding sites, so the most exciting and current research focus is centered on iron-dopamine dysfunction. Functional MRI (fMRI) points to locations in the brainstem, cerebellum, and thalamus. CSF analysis, special MRI, and neuropathological studies demonstrate reduction in CNS iron or ferritin or both. MBBSPPT.COM 15
Periodic Limb Movements in Sleep Periodic limb movements in sleep is a PSG finding. PLMS appears most commonly in RLS but may also occur in a other medical, neurological, and sleep disorders and with ingestion of medications (e.g., SSRIs, tricyclic antidepressants) Can occur in normal individuals, particularly in those older than age 65. Currently PLMD characterized by PSG findings of PLMS without associated RLS causing repeated awakenings and sleep fragmentations. There is a growing body of evidence that PLMS may simply be a PSG observation and may have no specific clinical significance MBBSPPT.COM 16
Features of Periodic Limb Movements in Sleep Repetitive, often stereotyped movements during NREM sleep. Usually noted in legs and consisting of extension of great toe, dorsiflexion of ankle, and flexion of knee and hip; sometimes seen in arms. Periodic or quasi-periodic at an average interval of 20-40 sec (range, 5-90 sec) with a duration of 0.5-10 sec and as part of at least 4 consecutive movements. Occurs at any age, but prevalence increases with age. May occur as an isolated condition or may be associated with a large number of other medical, neurological, or sleep disorders and medications. Seen in at least 80% of patients with restless legs syndrome. MBBSPPT.COM 17
Treatment Patients who present with RLS should, in addition to a thorough physical examination, also get a complete blood count and an iron level. It is generally recommended that ferritin level less than 50 mcg/l should be taken as a cut-off for treatment with oral iron. Caffeine, alcohol, nicotine and medications that aggravate RLS should be avoided. MBBSPPT.COM 18
Treatment Akpinar in 1982 accidentally came across the beneficial effects of levodopa on RLS. The most commonly used dopaminergic agents are levodopa, dopamine agonist such as ropinirole, pramipexole, pergolide. The efficacy of dopaminergic agents has been shown to be 90% in randomized placebo-controlled trials. MBBSPPT.COM 19
Treatment They are generally effective in not only relieving symptoms but also actually decreasing the number of movements at night. Levodopa/carbidopa generally works better for intermittent symptoms and as prophylaxis prior to car rides and plane trips. For daily symptoms, either ropinirole or pramipexole can be used. MBBSPPT.COM 20
Treatment They should be administered at least 2 hr prior to the onset of symptoms. For RLS symptoms that occur mostly in the early part of the night, taking these medications with dinner maybe helpful. In cases of PLMs, they should be given an hour prior to going to sleep. Both pramipexole and ropinirole can be started at 0.25 mg and increased as tolerated. The maximum dose of these medications is generally 3 mg. In patients who are intolerant to dopaminergic medications, the ergot- derivative pergolide can be used. The starting dose is a 0.025 mg and increased up to 0.5 mg. MBBSPPT.COM 21
Treatment Augmentation is the most common side effect with long-term use of levodopa in RLS. After initial improvement, symptoms worsen with use of Levodopa. Augmentation has also been reported with other dopaminergic agents and the incidence with these agents is probably around 20%. When augmentation occurs drug should be withheld rather than increased. MBBSPPT.COM 22
Treatment Stopping the medications usually result in rebound symptoms and that they can be managed effectively with benzodiazepine receptor agonists (zolpidem, zaleplon) . Antiepileptic agents such as gabapentin and lamotrigine have been effectively used as second line agents in the treatment of RLS. MBBSPPT.COM 23
Recommended Drug Management of Restless Legs Syndrome. Frequency or Quality of Symptoms First choice Second choice Third choice Nightly Dopamine agonist Opiates Gabapentin, sedative hypnotic agent Frequent (3 to 5 times per week) Sedative hypnotic agent Opiate Levodopa Occasional Levodopa Sedative hypnotic agent Opiates Painful Gabapentin, opiates Dopamine agonist Sedative hypnotic agent