Sentinel Events Registry Summary Report - Office of Analytics

Analysis of Sentinel Events Registry participation in Nevada healthcare facilities, data collection methods using REDCap platform, and reporting requirements for serious clinical events. The report highlights low participation rates and key findings from data analysis.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Joe Lombardo Governor Richard Whitley Director 2023 Sentinel Events Registry Summary Report Office of Analytics and Division of Public and Behavioral Health Jesse Wellman, Biostatistician II June 7, 2024 Department of Health and Human Services Helping people. It s who we are and what we do.
Agenda 1. Sentinel event definition 2. Who should report sentinel events? 3. Data collection methods 4. Data and analysis results 5. Plans and goals 6. Conclusion 2
What is a Sentinel Event? Defined as a serious reportable event. -largely preventable, and harmful clinical events that should never happen Events that are reportable are published by the National Quality Forum (NRS 439.830). NQF has announced a period of review regarding adverse event definitions. Healthcare Acquired Infections no longer reported to State SER, but Federally since 2013. Reporting has been conducted in Nevada since 2000, with force of statute since 2011. 3
Who should report a Sentinel Event? NRS 439.803 Health facility defined. Health facility means: 1. Any facility licensed by the Division pursuant to chapter 449 of NRS; and 2. A home operated by a provider of community-based living arrangement services, as defined in NRS 449.0026. (Added to NRS by 2019, page 1666) (Includes Medical facilities) 4
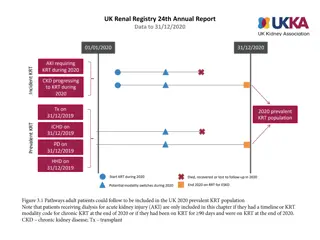
Data Collection Methods Using the Research Electronic Data Capture (REDCap) platform (projectredcap.org), patient safety officers or their designated reporters enter data, reporting on individual events, the annual summary report, and the facility s contact information. Individual Event Report Forms: Part 1 Initial report to sentinel events registry (notification), 14 days from event awareness Part 2 Factor areas, departments, and root cause analysis findings, 45 days after notification Summary Annual Report forms (Due March 1 for the previous calendar year): Summary Annual Report Form Patient Safety Plan (Medical facilities only) All health facilities are required to submit regardless if an event occurs Standardized list of reportable events as selection criteria, including category for non-natural death. 5
Data and Analysis results Sentinel Event Registry Participation by Healthcare Facility Type, 2023 There are 1,828 Licensed Health Facilities in the State of Nevada. Participation 225 facilities participated in at least one reporting mechanism of the SER 12% of all facilities participate. 63% of medical facilities participate. 175 facilities reported at least one individual event. 207 facilities filed an annual summary report. Key Findings Despite receiving email notification each year, participation remains low. The SER findings represent only 12% of the total health care facilities in Nevada. 6
Fall (40.3%) Sentinel Events From Individual Reports Pressure ulcer (stage 3 or 4 or unstageable) (19.4%) Elopement (disappearance) (4%) 22.9% 40.3% Procedure complication(s) (4%) 2.9% Unintended retained foreign object (3.4%) 3.1% 3.4% Burn (3.1%) 4.0% Physical Assault (2.9%) 4.0% All Other Events (22.9%) 19.4% 7
Fall 141 Pressure Ulcer 72 Surgery 37 Sentinel Events From Individual Reports Elopement 14 Self Harm Related 13 Medication error 13 Sexual Related 12 Physical Harm 11 Burn 11 Death - Other than Natural Causes 10 Retraint Related 5 Gas 5 Failure to Communicate 4 Specimen Related 3 Use of Contaminated 2 Discharge 2 Device 2 Intra- or post-operative death 1 Blood 1 Air embolism 1 0 20 40 60 80 100 120 140 160 8
0.9% Fall (56 %) 0.9% 1.0% Sentinel Events From Annual Reporting 7.3% 2.0% Pressure ulcer (all stages or unstageable) (33.8 %) Elopement (disappearance) (2 %) Procedure complication(s) (1 %) 56.0% 33.8% Physical assault (0.9 %) Medication error (wrong drug) (0.9 %) All Others (7.3 %) 9
Fall 1115 Pressure Ulcer 672 Sentinel Events From Annual Reporting Medication error 48 Elopement 39 Surgery 31 Self Harm Related 19 Sexual Related 8 Burn 7 Gas 4 Failure to Communicate 3 Device 2 Discharge 1 Air embolism 1 0 200 400 600 800 1000 1200 10
Factors Attributed 5.4% 1.5% Patient (45.9%) Contributing Factors to Events % 8.1% Staff (23.1%) Patient 45.9% Staff 23.1% Communication/Documentation (15.9%) Communication/Documentation 15.9% 15.9% 45.9% Organization Technical Environment Total (Percentages may not add up to 100% due to rounding) 8.1% 5.4% 1.5% Organization (8.1%) Technical (5.4%) 23.1% 100% Environmental (1.5%) 11
Safety Meetings Facilities Meetings NRS Expectation Monthly (>25 employees and contractors) or Quarterly (<=25 employees and contractors) Meetings Per NRS Expectation Total Facilities Percentage Yes 177 85.5% No (Non-Compliant) 27 13% Did Not Report 3 1.5% Total 207 100% 12
SER Event Lessons Learned From Lessons Learned Communication between all staff prior to the arrival of the patient leads to better outcomes. Invasive procedures benefit from a staff run down of the procedure before starting. Accidents can happen anytime. Staff are there to monitor and assist patients. There is no down time. Additional training for handling defiant patients and making all aware of escalation steps is needed. If staff fail to follow established policy, then the adverse outcome is what is expected. Staff is expected to thoroughly verify patient claims. Wound care is everyone s business. If you need help with a patient, call for help. Hero s call for help. Not calling for help puts everyone at risk. Being late by even by 2 minutes on routine checks can lead to adverse outcomes. Lack of hand-off communication is unacceptable. Verbal reports are not sufficient. Sending facility, receiving facility and transporter must all confirm level of care needed by the patient/resident. 13
SER Plans and Achievements Plans: A Sentinel Events Registry dashboard is in progress. Review the possibility of a survey link for the Annual Summary report. Could be completed even without registering to report individual events. Create a series of short instructional videos. Seek funding to provide mail notification, in addition to email notification regarding the Annual Summary report. Prepare a WhitePaper outlining the program and how it applies to certain health facility types that might be considered exempt by the facility but are not exempt per NRS. Will include language regarding NRS financial penalty sections, failure to participate. Achievements: Moved the Frequently Asked Questions, previously a pdf file, to an online link. (https://dpbh.nv.gov/Programs/SER/dta/FAQs/SER_Frequently_Asked_Questions/) Cleaned up data issues. 14
SER Annual Report Conclusion The Sentinel Events Registry focuses on helping health care facilities licensed by the Bureau of Health Care Quality and Compliance in identifying, and reporting serious, preventable incidents at their businesses. Every interaction seeks to raise patient safety awareness. The program is currently proactive, and not punitive. Reporting levels for the year 2023 were slightly better than previous years. Issues that continue revolve around participation rates, funding to send regular mail notifications, staffing help, and data collection improvements. Ultimately improving patient safety is the responsibility of all stakeholders in the health care system, and includes patients, providers, health professionals, organizations, and governments. 15
Contact Information Jesse Wellman Biostatistician II ser@health.nv.gov data@dhhs.nv.gov (775) 684-4112 https://dpbh.nv.gov/SER/ 16
Questions? 17






")