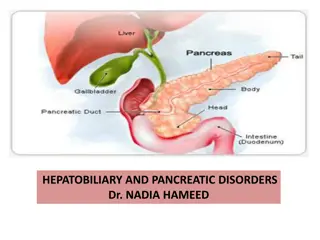
Sex and Gender Differences in Cirrhosis
This content discusses the sex and gender disparities in cirrhosis, highlighting differences in etiology, incidence, and mortality rates. It delves into the impact of factors like alcohol consumption, viral hepatitis, and obesity on the development of cirrhosis, providing insights into the epidemiological burden of the condition globally.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Submitted: August, 2023 Sex and Gender Differences in Cirrhosis
Sex and Gender Definitions and Proper Use Sex and Gender Differences in Cirrhosis
Sex and Gender Definitions and Proper Use1 Sex: Biological male/female/intersex XY or XX chromosomes Sex organs Hormones Gender: Socially constructed and enacted roles and behaviors Man/Woman/Other Masculine/Feminine Gender Non-Conforming Sex/Gender Definitions & Proper Use
Etiology Sex and Gender Differences in Cirrhosis
Historically, viral hepatitis has been the leading etiology for Chronic Liver Disease (CLD), but advances in prevention strategies and treatment have led to improvements.1 Risk factors: obesity and alcohol consumption Sex differences in etiology and frequency of complications of cirrhosis2 Etiology Incidence in Males vs. Females Males > Females Males > Females Females > Males Females > Males Alcohol Viral Autoimmune Other Etiology
Proportion of Cirrhosis Deaths by Disease Etiology1,2 Disease Cirrhosis Deaths, Male Cirrhosis Deaths, Female Hepatitis B Hepatitis C Alcoholic Liver Disease NASH/NAFLD Other* *includes cryptogenic, autoimmune, Wilson s disease, alpha-1 anti-trypsin deficiency, and hemochromatosis 31.5% 25.5% 24% 26.7% 27.3% 20.6% 7.7% 8% 11.3% 17.3% Etiology
Epidemiology Sex and Gender Differences in Cirrhosis
Cirrhosis is a leading cause of morbidity and mortality in the world.1 It is the 11th leading cause of death and was the 15th leading cause of morbidity worldwide in 2016. CLD accounted for 1.32 million deaths with two-third among males and one-third among females. Epidemiology
Reductions in CLD mortality rates are dependent on each country s approach to hepatitis prevention and treatment, IV drug use, alcohol consumption, and obesity rates. The absolute number of CLD cases is estimated to be around 1.5 billion worldwide. The most common causes are Non-Alcohol Fatty Liver Disease (NAFLD), HBV, HCV, and ALD. Epidemiology
Pathophysiology Sex and Gender Differences in Cirrhosis
Sex differences in the pathophysiology of the incidence and outcomes is not completely understood.1 Various mechanisms of sex hormones: Oxidative and metabolic pathways Differential gene transcription in response to injury Sex differences in immune regulation Pathophysiology
Aminotransferases is a group of liver enzymes that initiate the conversion of amino acids to -ketoglutarate.2 The enzymes commonly used as markers of liver disease are alanine aminotransferase (ALT) and aspartate transaminase (AST). Normal levels of ALT and AST are below 40 IU/L AST3 Males Females 14-20 IU/L 10-36 IU/L Pathophysiology
Anatomy Sex and Gender Differences in Cirrhosis
Male liver is 10.5 cm and weighs 1400-1500 g1 Female liver is 7 cm and weighs 1200-1400 g The liver is a sexually dimorphic organ that is responsive to sex hormones.2 The liver is a regenerating organ. Usually in the case of an excess loss of liver volume (LV) LV is affected by body physique, blood flow, hormones, and liver damage. Anatomy
LV in liver cirrhosis is lower than in a normal liver. Effects of how body physique and metabolism affect LV is not clear. Estrogen is a hepatotropic factor, which helps with liver regeneration. Male and female livers express different subsets of genes, which affect the liver s ability to metabolize certain drugs and hormones. Anatomy
Physiology Sex and Gender Differences in Cirrhosis
Males are more likely to experience ALD, while females show a more rapid progression to fibrosis.1 Fibrosis of this tissue can lead to cirrhosis. Alcohol absorption is faster in females than in males and females are more susceptible to both acute and chronic effects of alcohol when compared to males.2 Physiology
Females have slightly lower ALT and AST levels but have higher AST/ALT ratios compared to males.1 Estradiol may affect liver function through its action on estrogen receptor , which acts as a coordinator of energy metabolism in the liver. Fluctuations in estrogen affect the synthesis of fatty acids and cholesterol. Additionally, low estrogen levels have been linked to an increased risk of non-alcoholic fatty liver in both human and animal studies. Physiology
Gender affirming hormone therapy (GAHT) is expected to affect ALT and AST levels in transgender people.1 The effect of testosterone in liver function is less understood, but it is known that the liver contains androgen and estradiol receptors, and testosterone is converted to estradiol by aromatase in the liver. Both a lack of testosterone in males with hypogonadism and the excess of testosterone in females diagnosed with polycystic ovary syndrome increases the risk of non- alcoholic fatty liver disease and can result in abnormal levels of liver enzymes. Physiology
Clinical Presentation Sex and Gender Differences in Cirrhosis
Certain factors increase risk in both sexes:1 Overweight Drinking too much alcohol (more than two drinks per day for males and one drink per day for females) Diabetes Injecting drugs Unprotected sex Clinical Presentation
Some people have no symptoms while others present with: Pain and swelling in the abdomen Jaundice Fatigue Nausea or vomiting Itching Dark urine Light-colored stools Clinical Presentation
Females are more likely than males to have non-cirrhosis comorbidities but are less likely to have cirrhosis complications.2 Females more likely to have acute bacterial infections but less likely to have spontaneous bacterial peritonitis. Clinical Presentation
Presentation of cirrhosis includes presentation of the complications that occur during the disease course:1 Ascites Spontaneous bacterial peritonitis (SBP) Hepatorenal syndrome (HRS) Esophageal Varices Hepatic encephalopathy Treatment varies depending on which disease state is present Clinical Presentation
Pathogenesis Sex and Gender Differences in Cirrhosis
Sex Considerations Sex and Gender Differences in Cirrhosis
Ascites Sex and Gender Differences in Cirrhosis
Cirrhosis is the most common cause of ascites.1 Initial evaluation includes a history, physical exam, abdominal ultrasound, laboratory assessment of liver and renal function, serum and urine electrolytes, and a diagnostic paracentesis. Classification of Ascites: Grade 1: mild ascites only detectable by ultrasound Grade 2: manifested by moderate symmetrical distension of abdomen Grade 3: marked distension of the abdomen Ascites
Differences Between Sexes:1 Some females may have about 20 mL during their menstrual cycle. Females less likely to have ascites. Ascites
Treatment:1 Dietary sodium should be restricted to 2 grams/day. Aldosterone antagonists (spironolactone) and loop diuretics (furosemide, torsemide, bumetanide) are the mainstay of diuretic treatment. Recommended initial dose of spironolactone is 100 mg/day, which can be increased up to 400 mg/day. Initial dose of furosemide at 40 mg/day may be titrated according to response and tolerability to 160 mg/day. Ascites
Spontaneous Bacterial Peritonitis Sex and Gender Differences in Cirrhosis
Ascites can lead to SBP in about 10-20% of cases.1 SBP is caused by immunosuppression and migration of gram-negative intestinal bacteria. Clinical Presentation:1 Fever > 100 F in 50-80% of patients Worsening HE Hypotension in 5-15% Diffuse abdominal pain with rebound in 27-72% Spontaneous Bacterial Peritonitis (SBP)
Diagnosis:1 Diagnostic paracentesis (5-10 mL) Absolute polymorphonuclear neutrophil (PMN) count > 250/mm3 has the highest sensitivity of early diagnosis Treatment:1 First-line therapy is an IV 3rd generation cephalosporin for 5 days Spontaneous Bacterial Peritonitis (SBP)
Hepatorenal Syndrome Sex and Gender Differences in Cirrhosis
Also known as HRS-AKI (Type-1 HRS)1 Renal failure that occurs in patients with ascites and portal hypertension Late complication of cirrhosis that accounts for about 3.2% of all hospital discharges related to cirrhosis This can be worsened by decreased cardiac output in patients with cirrhosis-associated cardiomyopathy Systemic inflammation may trigger immune-mediated renal injury Hepatorenal Syndrome
Diagnosis:1 Increase in serum creatinine 0.3 mg/dL within < 48 hours 50% increase in serum creatinine from baseline within the preceding 7 days Treatment:1 Reversible factors (e.g., diuretics, NSAIDs, aminoglycosides, and ACE inhibitors), infection and sepsis, and GI bleeding 1.5 g/kg albumin on day 1 followed by 1 g/kg on day 3 Midodrine 5-15 mg every 8 hours Octreotide 100-200 mcg every 8 hours Hepatorenal Syndrome
Esophageal Varices Sex and Gender Differences in Cirrhosis
Condition1 Hematemesis Description Vomiting of red blood or coffee grounds Indicative of upper GI source Present in about 30% of patients; 50% with melena Black, tarry stool Blood present in the GI tract for at least 14 hours Present in 20% of patients; 30% with hematemesis Passage of bright red blood from rectum Indicative of lower GI source Present in 5% of patients Occult GI bleeding Examination of stool, identified in absence of bleeding Symptoms of blood loss or anemia Melena Hematochezia Light-headedness, syncope, fatigue, angina, dyspnea Esophageal Varices
Primary Prevention:1 Propranolol 20-40 mg twice daily Nadolol 20-40 mg once daily Carvedilol 6.25 mg once daily Therapy:1 Octreotide Endoscopic Variceal Band Ligation Transjugular Intrahepatic Portosystemic Shunt Esophageal Varices
Hepatic Encephalopathy Sex and Gender Differences in Cirrhosis
Pathophysiology:1 HE is due to a buildup of ammonia in the blood, which can get into the brain and cause dysregulation of glutamate and GABA metabolism. Presentation:1 Early signs include irritability, tremor, and later developments of somnolence, convulsions, and coma. Diagnosis:1 The West Haven criteria along with ammonia levels Hepatic Encephalopathy
Treatment:1 Discontinue HE-favoring drugs (diuretics, sedatives) Low-protein diet Acidification of feces with lactulose to increase ammonia excretion Neomycin Rifaximin shows efficacy with lactulose but very expensive Effective add-on therapy for prevention of recurrence Hepatic Encephalopathy
Sex Considerations Sex and Gender Differences in Cirrhosis
Females have lower rates of cirrhosis complications.1 Studies have shown that there is a male predominance of portal hypertensive complications. Hepatic encephalopathy more common in females. Sex Considerations
Females are less likely to be hospitalized with the typical complications of cirrhosis (e.g., ascites, variceal bleeding, and SBP) and are less likely than males to die during hospitalization.1 Males were younger and treated at large, urban and teaching hospitals. Gender affirming hormone therapy (GAHT) on liver enzymes alanine aminotransferase (ALT) and aspartate transaminase (AST) is an area of uncertainty in transgender health.2 Social Considerations
Transgender males might increase ALT and AST levels following testosterone initiation; however, the clinical significance of this association is still unclear. Feminizing GAHT is unlikely to cause changes in liver enzyme levels. Social Considerations
Summary Sex and Gender Differences in Cirrhosis
The liver is a regenerating organ Estrogen is a hepatotropic factor Differences between sexes in regards to presentation and occurrence in complications Unknown why these differences are present Summary


















 is expected")

















1")