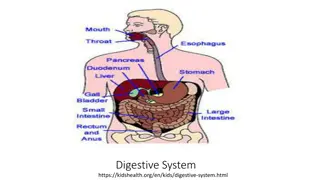
The gallbladder
The gallbladder, cystic duct, and common bile duct play vital roles in the storage and release of bile for digestion. Understanding their anatomical divisions and functions is crucial for medical professionals. This article covers the dimensions, structure, and physiological processes of these components, shedding light on their interconnected roles within the digestive system.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
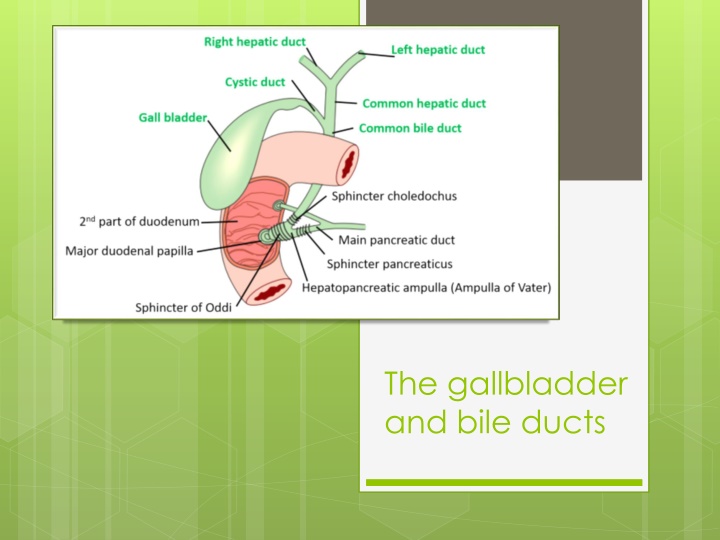
The gallbladder and bile ducts
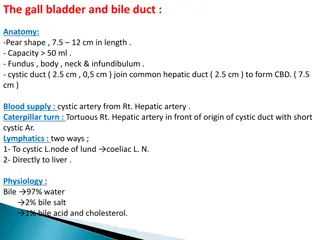
SURGICAL ANATOMY AND PHYSIOLOGY OF GALLBLADDAR It is a pear-shaped structure, 7.5 12 cm long, with a normal capacity of about 25 30mL. The anatomical divisions are a fundus, a body, a neck AND infundibulum.
The cystic duct is about 3cm in length but the length is variable. The lumen is usually 1 3mm in diameter. The mucosa of the cystic duct is arranged in spiral folds known as the valves of Heister.
COMMON BILE DUCT The common hepatic duct is usually less than 2.5 cm long and is formed by the union of the right and left hepatic ducts. The common bile duct is about 7.5cm long and formed by the junction of the cystic and common hepatic ducts. It is divided into four parts: 1. the supraduodenal portion, about 2.5 cm long, runs in the free edge of the lesser omentum. 2. the retroduodenal portion. 3. the infraduodenal portion lies in a groove, but at times in a tunnel, on the posterior surface of the pancreas. 4. the intraduodenal portion passes obliquely through the wall of the second part of the duodenum, where it is surrounded by the sphincter of Oddi, and terminates by opening on the summit of the ampulla of Vater.
Surgical physiology Bile is produced by the liver and stored in the gallbladder, from which it is released into the duodenum. As it leaves the liver it is composed of 97% water, bile salts, phospholipids, cholesterol and bilirubin. The liver excretes bile at a rate estimated to be approximately 40mL/hour. About 95% of bile salts are reabsorbed in the terminal ileum (enterohepatic circulation).
Functions of the gallbladder The gallbladder is a reservoir for bile. During fasting, resistance to flow through the sphincter of Oddi is high, and bile excreted by the liver is diverted to the gallbladder. After feeding, the resistance to flow through the sphincter is reduced, the gallbladder contracts and the bile enters the duodenum. These motor responses of the biliary tract are in part affected by the hormone cholecystokinin
Functions of the gallbladder the gallbladder is concentrated of bile by absorption of water, sodium chloride and bicarbonate via the mucous membrane of the gallbladder. the gallbladder is the secretion of mucus approximately 20mL is produced per day. With complete obstruction of the cystic duct in an otherwise healthy gallbladder, a mucocoele may develop as a result of ongoing mucus secretion by the gallbladder mucosa.
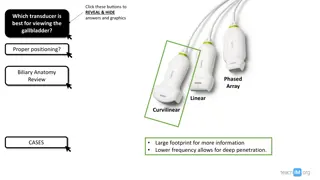
Radiological investigation of the biliary tree Plain radiograph: calcification, air within biliary system Ultrasound: stones and biliary dilatation MRCP: anatomy and stones CT scan: anatomy, liver, gallbladder and pancreatic cancer Radioisotope scanning (HIDA scan): function ERCP: anatomy, stones and biliary strictures PTC: anatomy and biliary strictures EUS: anatomy, stones
GALLSTONES(CHOLELITHIASIS) Gallstones are the most common biliary pathology. Affect 10 15% of the population in Western societies. They are asymptomatic in the majority of cases (>80%). In the UK, the prevalence of gallstones at the time of death is estimated to be 17% and may be increasing. Approximately 1 2% of asymptomatic patients will develop symptoms requiring surgery per year, making cholecystectomy one of the most common operations performed by general surgeons
Types of Gallstones Gallstones can be divided into three main types: Cholesterol stone. Pigment (brown/black). Mixed stones. In the USA and Europe 80% are cholesterol or mixed stones, whereas in Asia 80% are pigment stones. Cholesterol or mixed stones contain 51 99% pure cholesterol plus calcium salts, bile acids, bile pigments and phospholipids. 1. 2. 3.
Causes of Gallstone Obesity, high-caloric diets and certain medications (e.g. oral contraceptives) can increase secretion of cholesterol and supersaturate the bile, increasing the lithogenicity of bile. Resection of the terminal ileum, which diminishes the enterohepatic circulation, will deplete the bile acid pool and result in cholesterol supersaturation. Nucleation of cholesterol crystals from multilamellar vesicles is a crucial step in gallstone formation. Abnormal emptying of the gallbladder may aid the aggregation of nucleated cholesterol crystals.
Pathogenicity of stones Pigment stone is the name used for stones containing <30% cholesterol. There are two types: black and brown. Black stones are largely composed of an insoluble bilirubin pigment mixed with calcium phosphate and calcium bicarbonate. Overall, 20 30% of stones are black. The incidence rises with age. Black stones are associated with haemolysis, usually hereditary spherocytosis or sickle cell disease. For reasons that are unclear, patients with cirrhosis have a higher instance of pigmented stones.
Brown pigment stones contain calcium bilirubinate, calcium palmitate and calcium stearate, as well as cholesterol. Brown stones are rare in the gallbladder. They form in the bile duct and are related to bile stasis and infected bile. Stone formation is related to the deconjugation of bilirubin. Brown pigment stones are also associated with the presence of foreign bodies within the bile ducts such as endoprostheses (stents) or parasites such as Clonorchis sinensis and Ascaris lumbricoides.
Effects and complications of gallstones 1. Biliary colic 2. Acute cholecystitis 3. Chronic cholecystitis 4. Empyema of the gallbladder 5. Mucocoele 6. Perforation 7. Biliary obstruction 8. Acute cholangitis 9. Acute pancreatitis 10. Intestinal obstruction (gallstone ileus)
Differential diagnosis of acute cholecystitis Common Appendicitis Perforated peptic ulcer Acute pancreatitis Rare Acute pyelonephritis Myocardial infarction Pneumonia right lower lobe 1. 2. 3. 1. 2. 3.
EMPYEMA OF THE GALLBLADDER Empyema may be a sequel to acute cholecystitis or the result of a mucocoele becoming infected. The gallbladder is distended with pus. The optimal treatment is drainage (cholecystostomy) and, later, cholecystectomy.










")