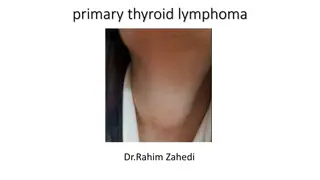
Thyroid Disorders - Diagnosis and Management
Thyroid disorders like Graves' disease can present with various symptoms and require careful assessment for accurate diagnosis. While thyroid ultrasound may not be essential for diagnosing Graves' disease specifically, it plays a crucial role in managing thyroid nodules. The Endocrine Society of Australia emphasizes thoughtful evaluation and appropriate follow-up for patients with thyroid abnormalities.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Is Thyroid USS a must? Endocrine Society of Australia
Fatima Patient medical history (PMHx) 34-year old female Previously fit and healthy Symptoms Palpitations Sweating 10 kg weight loss in the last 2 months Irregular period in the last 2 months
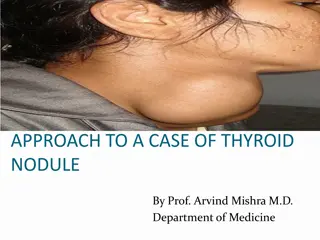
Patient Name Examination BP 106/70, HR 86/min, regular nil lid lag or ophthalmoplegia or proptosis diffusely enlarged butterfly-shaped swelling in neck, moves with swallowing, non-tender Nil thyroid bruit mild fine tremors nil clubbing Absent Pemberton s sign brisk reflexes nil proximal myopathy nil pretibial myxedema Tests / Investigations TSH < 0.05 mIU/L (0.5-4.5) Free T4 33 pmol/L (7-18) Free T3 12 pmol/L (3.5-6) TSH receptor Ab 8.8 IU/L (<1.8)
What is the diagnosis? Thyroiditis Toxic nodule Graves disease Multinodular goitre
Question Thyroiditis Toxic nodule Graves disease Multinodular goitre
Graves disease Graves disease should be suspected in patients presenting with signs and symptoms of thyrotoxicosis (tachycardia, weight loss or poor weight gain, and lid lag, often with tremor and neuropsychiatric symptoms) A significant share of these patients will have goitre and ophthalmopathy. The diagnosis of Graves disease as the cause of the thyrotoxicosis is confirmed by the presence of thyrotropin receptor antibodies (TSHR-Ab), which are detectable in the majority A positive thyroid-stimulating immunoglobulin (TSI) confirms the presence of a thyrotropin receptor (TSHR)-stimulating antibody.
Is Thyroid USS essential to diagnose Graves disease? It is not essential if there is no asymmetrical or nodular enlargement on examination Assessment with thyroid USS would significantly influence decision-making on management of thyroid nodules, but not for Graves disease Appropriate follow-up management plan is needed when thyroid nodules are detected
Evolve Recommendation Don t routinely order a thyroid ultrasound in patients with abnormal thyroid function tests if there is no nodular abnormality of the thyroid gland The Endocrine Society of Australia Evolve is facilitated by the Royal Australasian College of Physicians
What is best practice? What are some common uses of thyroid ultrasound? An ultrasound of the thyroid is typically used: to analyse the appearance of thyroid nodules and determine if they are the more common benign nodule or if the nodule has features that require a biopsy. If biopsy is required, ultrasound guided needle aspiration can help improve accuracy of the biopsy. to look for additional nodules in patients with one or more nodules felt on physical exam to see if a thyroid nodule has substantially grown over time
What is best practice? What are the limitations of thyroid ultrasound? Incidentally discovered thyroid nodules on ultrasound are common. Overzealous use of ultrasound will frequently identify nodules, which are unrelated to the abnormal thyroid function, and may divert the clinical evaluation to assess the nodules, rather than the thyroid dysfunction, which may lead to further unnecessary investigations, unwarranted patient anxiety and increased costs. Imaging may be needed in thyrotoxic patients; when needed, a radionuclide thyroid scan, not an ultrasound, is used to assess the etiology of the thyrotoxicosis and the possibility of focal autonomy in a thyroid nodule or nodules.
References https://evolve.edu.au/recommendations/esa https://www.radiologyinfo.org/en/info.cfm?pg=us-thyroid Thyrotoxicosis and hyperthyroidism, Therapeutic Guidelines
How this case study was made This case study was developed by Dr Su Win Htike as a member or the RACP Evolve Policy Reference Group. This case study has been reviewed by the RACP Evolve Policy Reference Group in particular Prof Jane M Andrews, the Australian Diabetes Society, the Endocrine Surgery section of the Royal Australasian College of Surgeons, and NPS MedicineWise. This case study was approved for publication by the Endocrine Society of Australia Medical Affair Committee in August 2020.
Evaluation How likely is this Evolve recommendation to change your practice? 1. Not at all 2. Somewhat 3. Significantly Explain your reasoning
About Evolve As part of a global movement, Evolve is a flagship initiative led by physicians, specialties and the Royal Australasian College of Physicians (RACP) to drive high-value, high-quality care in Australia and New Zealand. Evolve aims to reduce low-value care by supporting physicians to: be leaders in changing clinical behaviour for better patient care make better decisions, and make better use of resources. Find out more: www.evolve.edu.au Get in touch: evolve@racp.edu.au