Tower Hamlets Primary Care Pilot Pathways for Unscheduled Care
Explore the innovative primary care pathways for unscheduled care in Tower Hamlets, including referral processes, clinical assessments, and coordination with secondary care services. Learn about the current and proposed models via the REACH system, aimed at enhancing patient experiences and outcomes.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
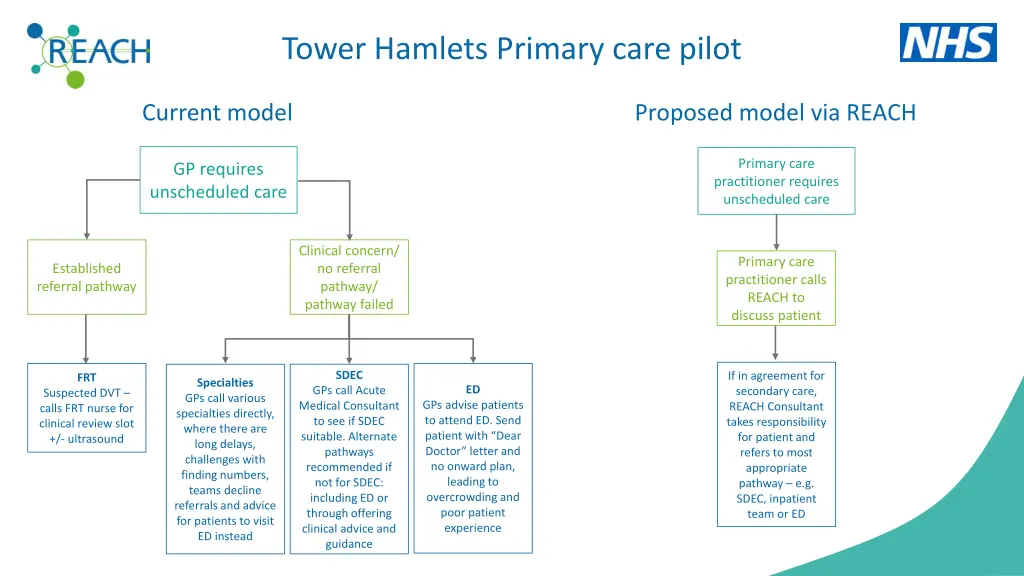
Tower Hamlets Primary care pilot Current model Proposed model via REACH Primary care practitioner requires unscheduled care GP requires unscheduled care Clinical concern/ no referral pathway/ pathway failed Primary care practitioner calls REACH to discuss patient Established referral pathway SDEC If in agreement for secondary care, REACH Consultant takes responsibility for patient and refers to most appropriate pathway e.g. SDEC, inpatient team or ED FRT Specialties GPs call various specialties directly, where there are long delays, challenges with finding numbers, teams decline referrals and advice for patients to visit ED instead ED GPs call Acute Medical Consultant to see if SDEC suitable. Alternate pathways recommended if not for SDEC: including ED or through offering clinical advice and guidance Suspected DVT calls FRT nurse for clinical review slot +/- ultrasound GPs advise patients to attend ED. Send patient with Dear Doctor letter and no onward plan, leading to overcrowding and poor patient experience
Inclusion criteria: Seen face to face by primary care Requires unscheduled care: including speciality review (not advice), ED review or other secondary care Over 16 years old Ambulant + can make own way to hospital Patients who have had a home visit, are frail/complex and where enhanced assessment may support community management (accessing PRU via SPA) Patients with learning disabilities requiring secondary emergency care Exclusion criteria: Not seen face to face Requiring time critical 999 ambulance response Primary mental health presentations Seeking speciality clinical advice Patients in labour or obstetric emergencies Children under 16 years old Medication requests Referrals into outpatient services Radiology requests
Suggested example pathways Presentation from Primary Care (in GP surgery or at home) Current Pathway Future Pathway Suspected cardiac chest pain Acute / ongoing pain call 999/LAS Discrete episode of pain, no current symptoms send to ED Call REACH to risk assess and co-ordinate. Needs discussion with consultant Suspected DVT (lower limb, below knee) Send to ED Mon-Fri 0800-1700 stream to SDEC. Other hours will be streamed to UTC if mobile. Call REACH to co-ordinate to SDEC. Could be managed by nurse + junior clinician Suspected PE Send to ED streamed as per streaming tool. Call 999/LAS if abnormal physiology. Call REACH to risk assess and co-ordinate to most appropriate area. Hyperemesis gravidarum Send to ED as per streaming pathway (usually ED then SDEC). Call REACH to co-ordinate access to SDEC/CDU. DKA Send to ED as per streaming pathway. Call 999/LAS if abnormal physiology. Call REACH to co-ordinate response. Suspected TIA Call REACH to co-ordinate response. Headache ?SAH Send to ED to stream as per headache pathway. Call REACH to -co-ordinate SDEC/CDU. Cauda equina syndrome Send to ED, stream to ED, ED team arrange MRI in and out of hours then ED d/w Spinal on-call. 999/LAS if unable to self-present state cauda equina as this will be blue-lighted to ED as per LAS policy. Call REACH to co-ordinate SDEC/CDU and MRI request. Acute pelvic pain Call EGU (Gynae SDEC) Mon-Fri 0800-1800, Sat 0930-1300. 02035941579. Otherwise send to ED for streaming, imaging and bloods. Call REACH to risk assess and co-ordinate Mastoiditis / severe ear infection Send to ED for imaging / bloods. Call REACH to co-ordinate response imaging, bloods and SDEC. Ureteric colic Send to ED stream as per streaming tool then imaging in SDEC. Call REACH to co-ordinate imaging / SDEC. Acutely unwell / febrile oncology pt. Call Chemo hotline consider PRU response in community, or Cancer Assessment Unit (Cancer SDEC). Otherwise ED with patient to inform staff about chemotherapy. Call Chemo hotline to co-ordinate care.
Face-to-face review of patient by primary care ED review, SDEC, speciality review, other secondary care or access to PRU = Meets inclusion criteria for SPA via REACH Phone call to REACH SPA 0203 137 5604 Booked in as normal DSE process referral source GP remains the same Patient discussed with REACH consultant +/- video consultation with junior clinician Patient details passed to nurse to coordinate SDEC with junior clinician OR Onward referral managed by REACH team (unless decision made for care to remain under primary care) REACH book to SDEC/UTC/ED as appropriate +/- referral to speciality Discharge summary completed as normal
Feedback Primary care feedback to REACH REACH feedback to primary care Email bartshealth.reachshiftleaders@nhs.net Include GP practice, date of referral/case, patient details and any other relevant details This will be passed on to REACH leads, or if urgent, to duty REACH team. Typically via discharge summary (ED/SDEC/UTC). Any specific feedback? Suggest email GP practice/practitioner directly? Including date of referral/case, patient details and any other relevant details Any concerns/specific feedback that is not felt to be appropriate following the above methods, to be emailed to Katy Hannaford and Alex Alexiou