Understanding Eating Disorders: Impacts and Behaviors
Explore the high morbidity and mortality rates associated with eating disorders, focusing on anorexia and bulimia. Learn about the rise of eating disorders, signs of probable growth and nutrition problems, and red flags for further assessment.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Standardizing Eating Disorders Care Vancouver Island: Medical Assessment & Monitoring REFERENCE SLIDES Corene Boe MD, Lorelei Johnson MD, Marilee Pumple RD
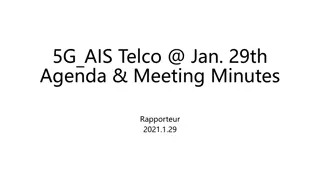
High morbidity and mortality High morbidity and mortality Mortality rates: Anorexia 9-20% (highest mortality rate of all Mental Health conditions); Bulimia 3% 4x increased risk of completed suicide Death from AN is >12x higher than any other chronic illness in 15-24 year old females Life expectancy reduction of 20-25 years for chronic AN Eating disorders are on the rise Eating disorders are on the rise Particularly in youth (estimates of 300-400% increases) More inpatient admissions for medical instability/higher acuity
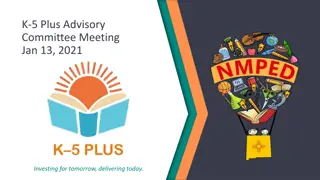
Very strong likes and dislikes around tase, texture, smell, and/or presentation of foods: Refusal to try new foods Limited variety (whole food groups excluded; brand-specific preferences) and very restricted number of foods (<20) Preferred foods can be dropped from diet Probable growth and/or nutrition problems Probable disruption to daily living (separate meal from family; not eating with peers; not eating at restaurants; frequent tantrums at mealtime) May be afraid of vomiting or choking on food Possible history of feeding problems in infancy (with breastfeeding; reflux; regurgitation; gagging) Red flags for further assessment: Some type of skill deficit (motor and/or oral-motor) Used to eat normally, but now extremely worried about germs, vomiting or choking Strong preferences: - taste, texture, preparation Limited variety - often excluding a food/texture category 1. 1. 2. Restricted number of foods (~20-30) Avoidance of new foods 3. 2. 3. 4. 4. Picky Eating Resource: 5. ELLYN SATTER S DIVISION OF RESPONSIBILITY IN FEEDING 6.
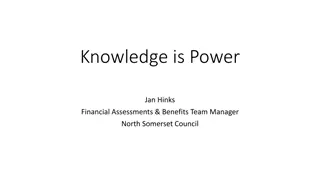
CLINICAL PATHOPHYSIOLOGY MONITORING TREATMENT OPTIONS DEPLETED GLUCOSE STORES, INCLUDING LIVER GLYCOGEN STORES 2 HR POSTPRANDIAL BG AND AM FASTING GLUCOSE, IF RECURRING LOW RANDOM GLUCOSE ON LABS INCREASE SNACKING FREQUENCY INCREASE PROTEIN CONTENT IN MEALS LOW BLOOD GLUCOSE SHIFTING PHOSPHATE RISK OF SEIZURE, COMA POST-PRANDIAL SW ELLING IN THE SETTING OF RESTRICTIONS (AT RISK FOR REFEEDING SYNDROME) NAPHOS SOLUTION 5 ML BID (PHOSLAX) OR PHOSPHATE 500 MG PO BID REFEEDING EDEMA PLUS THIAMINE 100 MG PO DAILY X1-2 W EEKS RISK OF ARRHYTHMIA LABS 1-3X PER W EEK FOR FREQUENT PURGING K+ LYTE 25MEQ FASTER ABSORBING; 1-4X/DAY K+ ELIXER20MEQ/15ML LIQUID OPTION; 1-3X/DAY K+ DUR 20-40 MEQ LARE ORANGE TABS SLOW K+ 8 MEQ SMALL TABS, NOT READILY ABSORBED HYPOKALEMIA ***ADD MAGNESIUM SUPP*** LOW W HOLE BODY STORES EVEN IF LAB VALUE N, CANT REPLACE K+ W ITHOUT REPLETING MG2+ MAGNESIUM ROUGIER 15 ML PO TID (SE: GI UPSET, LOOSE STOOLS) IV SUPP 5G MGSO4 (20MMOL) IN 250CC NS IV OVER 3 HRS (FOR RECURRENT HYPOKALEMIA, REPEAT ABOVE IV DOSE DAILY X5 DOSES) LOW INTAKE SLOW S TRANSIT TIME SYMPTOMS MANAGEMENT REGULAR MEALS FRUITLAX (NATURAL FRUIT JAM W ITH LAXATIVE PROPERTIES) PEG 3350 17G DAILY QID BOWEL CARE CHRONIC CONSTIPATION MAGNOLAX 40ML PO DAILY CASCARE 30ML PO DAILY DOCUSSATE 100 MG PO BID LAXATIVE ABUSE LEADS TO DEPENDENCE
https://keltyeatingdisorders.ca/wp-content/uploads/2017/05/Eating-Disorders-Toolkit-for-PCP-2018.pdfhttps://keltyeatingdisorders.ca/wp-content/uploads/2017/05/Eating-Disorders-Toolkit-for-PCP-2018.pdf https://keltyeatingdisorders.ca/wp-content/uploads/2017/05/Eating- Disorders-Toolkit-for-PCP-2018.pdf https://keltyeatingdisorders.ca/wp-content/uploads/2017/05/Eating-Disorders-Toolkit-for-PCP-2018.pdf https://keltyeatingdisorders.ca/wp-content/uploads/2017/05/Eating-Disorders-Toolkit-for-PCP-2018.pdf
http://www.lookingglassbc.com/residential-care https://www.childhealthbc.ca/sites/default/files/BCCH_ED_%20Pedatric%20Eating%20Disorders.pdf
https://mh.providencehealthcare.org/sites/default/files/ER%20guidelines.pdf https://mh.providencehealthcare.org/sites/default/files/ER%20guidelines.pdf https://mh.providencehealthcare.org/sites/default/files/ER%20guidelines.pdf https://www.childhealthindicatorsbc.ca/sites/default/files/BCCH_ED_%20Pedatric%20Eating%20Disorders.pdf https://www.childhealthindicatorsbc.ca/sites/default/files/BCCH_ED_%20Pedatric%20 Eating%20Disorders.pdf https://www.childhealthindicatorsbc.ca/sites/default/files/BCCH_ED_%20Pedatric%20Eating%20Disorders.pdf https://mh.providencehealthcare.org/sites/default/files/BC%20Eating%20Disorders% 20Clinical%20Practice%20Guidelines.pdf
https://balancedviewbc.ca/new_to_site.html https://learninglinksbc.ca/
keltyeatingdisorders.ca https://www.feast-ed.org/ https://keltyeatingdisorders.ca/recovery/meal-support/ ED-Parent-Caregiver-support.pdf (islandhealth.ca) peer-support-for-clients-with-eating-disorders.pdf (islandhealth.ca) https://eatcakepod.home.blog/ https://jessieslegacy.com/
keltyeatingdisorders.ca UpToDate Admissions guidelines developed with local and provincial eating disorder specialists including Internal Medicine, Psychiatry, Pediatrics, Dietitians, Family Physicians and ED Interdisciplinary treatment teams. Luck, A.J., et al. (2002), The SCOFF questionnaire and clinical interview for eating disorders in The SCOFF questionnaire and clinical interview for eating disorders in general practice : comparative study general practice : comparative study, British Medical Journal, (325) 7367; p755-756 Klein DA et.al. Eating Disorders in Primary Care: Diagnosis and Management. Eating Disorders in Primary Care: Diagnosis and Management. American Family Physician. 2021 Jan 1; 103(1); p22-34. Seferovic, A et.al. What is the best screening tool for eating disorders in the primary care What is the best screening tool for eating disorders in the primary care setting? setting? Evidence-Based Practice: March 2019; 22(3); p12 Hisham MM et. al. Refeeding syndrome: what it is, and how to prevent and treat it. Refeeding syndrome: what it is, and how to prevent and treat it. British Medical Journal. 2008 Jun 28; 336(7659): p1495-1498.