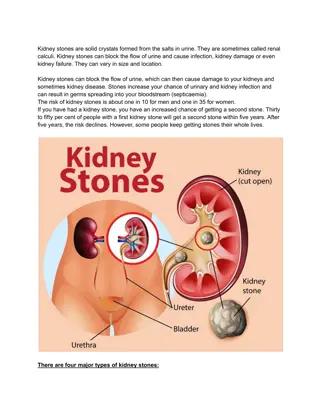
Understanding Kidney Pathology and Infections
Explore the pathology of the kidneys, including tumors and infections such as pyelonephritis. Learn about kidney features, urinary tract obstruction, and complications like necrosis. Understand chronic pyelonephritis and reflux nephropathy, with insights into diagnosis and treatment options.

Uploaded on | 1 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Pathology of the kidneys TIN Kidney tumors
Plan Urinary tract infection TIN tubulointerstitial nephritis Tumors
Kidney features 150gm: each kidney 1700 liters of blood filtered 180 L of G. filtrate 1.5 L of urine / day. Kidney is a retro-peritoneal organ Blood supply: Renal Artery & Vein One half of kidney is sufficient reserve
Pyelonephritis and Urinary Tract Infection Most commonly with E.coli Mostly ascending Main symptoms are fever and pain Most commonly at women Patients with catheters and malformations
Clinics obstruction of urinary tract, VUR, anamnesis of cathetrisation, diabetes, immunodeficit abrupt onset pain in costovertebral angle dysuria, polakisuria fever, malaise urinanalysis: pyuria (+ leukocytar casts), bacteriuria, hematuria frequent recurrences chronic form healing postpyelonephritic scars (fibrosis, chronic onflammation)
Complications necrosis of papils in diabetes, coagulative necrosis, dystrophic calcification pyonephrosis accumulation of pus in renal pelvis or uteter urinary tract obstruction perinephric abscesus propagation of purulent inflammation over the capsula in perirenal fat sepsis
Chronic Pyelonephritis and Reflux Nephropathy chronic inflammation and fibrosis of interstitium tubular atrophy thyroidisation periglomerular fibrosis, collaps of tufts sclerosis renovascular hypertension CRF, end-stage kidney
Chronic Pyelonephritis and Reflux Nephropathy
TIN Acute inflammation involving tubulointerstitial compartments Might be associated with acute tubular injury or tubulointerstitial scarring Common etiologies include drug, autoimmune, infection, hereditary and idiopathic
Tubulointerstitial Nephritis Induced by Drugs and Toxins
TIN sulfonamids, methicilin, ampicilin, rifampicin, thiazid, NSAID, allopurinol 2 weeks after application fever, eosinophilia, skin exantema renal injury (hematuria, proteinuria, incr. kreatinin) interstitial edema, inflammatory cells with eosinophils There is granulomatous and IG-4 variants 1) acute renal failure (ATN) 2) acute tubulointerstitial nephritis hypersensitive nephritis 3) chronic tubular injury CHRI
Metanephric tumors Metanephric adenoma Metanephric adenofibroma Metanephric stromal tumor Kidney Tumors Renal cell tumors Clear cell renal tumors Renal mesenchymal tumors Adult renal mesenchymal tumors Classic angiomyolipoma / PEComa of the kidney Epithelioid angiomyolipoma / epithelioid PEComa of the kidney Renal hemangioblastoma Juxtaglomerular cell tumor Renomedullary interstitial cell tumor Pediatric renal mesenchymal tumors Ossifying renal tumor of infancy Congenital mesoblastic nephroma Rhabdoid tumor of the kidney Clear cell sarcoma of the kidney Clear cell renal cell carcinoma Multilocular cystic renal neoplasm of low malignant potential Papillary renal tumors Renal papillary adenoma Papillary renal cell carcinoma Oncocytic and chromophobe renal tumors Oncocytoma of the kidney Chromophobe renal cell carcinoma Collecting duct tumors Collecting duct carcinoma Embryonal neoplasms of the kidney Nephroblastic tumors Nephrogenic rests Cystic partially dedifferentiated nephroblastoma Nephroblastoma Other renal tumors Clear cell papillary renal cell tumor Mucinous tubular and spindle cell carcinoma Tubulocystic renal cell carcinoma Acquired cystic disease associated renal cell carcinoma Mixed epithelial and stromal renal tumors Mixed epithelial and stromal tumor of the kidney Pediatric cystic nephroma Eosinophilic solid and cystic renal cell carcinoma Renal cell carcinoma NOS
Benign Tumors Renal Papillary Adenoma Angiomyolipoma Oncocytoma Juxtaglomerular cell tumor
Renal Papillary Adenoma Papillary adenoma is a benign kidney lesion Incidentally found in nephrectomies removed for larger tumors or other causes More common in kidneys harboring papillary RCC (> 25%), compared with other types of renal tumors Very common in end stage kidneys Change allows for increased acceptance of donor kidney for transplantation, in which kidneys with papillary lesions 15 mm would not be rejected
Angiomyolipoma Member of perivascular epithelioid cell (PEC) tumor family Angiomyolipoma, classic variant, is a benign mesenchymal neoplasm composed of admixture of thick dysmorphic blood vessels, smooth muscle and adipose tissue Amount of each component is variable Some cases show significant sclerosis Epithelioid variant has potential to metastasize Angiomyolipoma can occur in extrarenal sites Tumors can be quite large, multifocal and can extend into the renal vein or vena cava Classic variant is benign but may be complicated by hemorrhage if the tumor is large
Oncocytoma Renal oncocytoma are benign renal oncocytic neoplasms Essential to differentiate from mimicker oncocytic renal cell carcinoma entities Multiple tumors can be associated with syndromic conditions Usually asymptomatic; detected incidentally on imaging for unrelated reasons Rarely presents with hematuria and dysuria Well circumscribed lesion with central scar; usually no pseudocapsule, tumor directly abuts the renal parenchyma
Juxtaglomerular cell tumor Rare renin secreting tumor arising from the specialized smooth muscle cells of the glomerular afferent arteriole in the renal juxtaglomerular apparatus Occurs mostly in young adults; female predominance Frequently associated with severe and poorly controlled hypertension, hypokalemia and hyperaldosteronism secondary to tumor renin secretion Almost always benign with single case of metastatic disease Grossly well circuscribed nodule Micro: Glomoid appearance with sheets of polygonal to spindle cells with well defined cell border
Malignant Tumors Renal cell tumors Clear cell renal cell carcinoma Papillary renal tumors Papillary renal cell carcinoma Oncocytic and chromophobe renal tumors Chromophobe renal cell carcinoma Collecting duct tumors Collecting duct carcinoma Embryonal neoplasms of the kidney Nephroblastoma
Clear cell renal cell carcinoma Most common renal epithelial tumor, typically with clear cytoplasm and a compact nested or acinar growth pattern, intersected by delicate vasculature and with characteristic alterations to chromosome 3p involving VHL (von Hippel- Lindau) gene inactivation Cortical mass with golden yellow variegated cut surface Diverse architecture, primarily solid and nested Clear or granular eosinophilic cytoplasm and prominent but delicate capillary network > 95% sporadic, mostly single mass, sixth to seventh decade Metastases: Hematogenous more common: lung (most common), bone, liver, pleura, CNS, head and neck Lymphatic less common: hilar, aortic, caval and thoracic lymph nodes Extension into the renal sinus the most common pathway of spread, usually involving extension within the renal vein
Papillary renal cell carcinoma Usually circumscribed malignant neoplasm characterized by predominantly papillary or tubulopapillary architecture Usually asymptomatic; incidental finding on imaging Maybe multifocal or bilateral in chronic kidney disease and hereditary PRCC (germline MET mutation) Homogenous, solid mass with relative hypovascularity compared to nonpapillary RCC; may have cystic change and calcifications
Chromophob carcinoma Third most common renal cell carcinoma (RCC) subtype; 7% of adult renal epithelial tumors Majority are sporadic and incidental, no gender preference Mean age 58 years Solid sheet-like architecture
Sharply defined cell membranes (plant-like) Perinuclear halos (koilocytic)
Collecting duct carcinoma Rare (< 1% of kidney cancers) aggressive carcinoma of renal medulla arising from the principal cells of the distal collecting ducts of Bellini Morphology: irregular, infiltrating tubules with high grade cells often containing mucin; marked stromal desmoplasia and inflammatory infiltrate Essentially a diagnosis of exclusion
Nephroblastoma Nephroblastoma (or Wilms tumor) is a malignant embryonal tumor originating from nephrogenic blastema, which imitates the histology of developing kidney Primarily occurs in children Tumor consists of blastemal, epithelial and stromal elements (triphasic) which can be present in variable amounts Biphasic and monophasic tumors are not infrequent Epithelial and stromal elements may show different lines and degrees of differentiation (from poor to well differentiated) Most common: 3 - 4 years of age Slight female preponderance Majority of patients with Wilms tumor are nonsyndromic Relapses occur in ~15% of children, the majority within 2 years of diagnosis Usually presents as abdominal mass with no associated symptoms Other signs or symptoms (present in 20 - 30% of cases): Abdominal pain Hematuria Hypertension Anemia
Blastema, the least differentiated component Epithelial component
Necrosis component Stromal component




































")
")