Explore the symptoms and signs of Myasthenia Gravis in a clinical case scenario. Learn about the causes, investigations, differential diagnosis, and treatment options for this autoimmune neuromuscular condition affecting muscle strength and function.
Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
Case 1: Myasthenia Gravis A 30 year-old female came to the emergency complaining of difficulty in swallowing and in taking her breath. She stated that for past few months, she had progressive easy fatigability of eye muscles on watching TV. Also she become easily tired on caring about her house. Her symptoms improved by rest (or sleep) Examination of the patient revealed: - Drooping of upper eye lid of both eyes (ptosis). - Recurrent double vision (diplopia). - Difficulty in breathing (dypsnea). - Weakness and slight atrophy of facial, respiratory and upper limb muscles.
Case 1: Myasthenia Gravis - Cardiovascular examinations were normal. - Examination of other systems did not detect any abnormalities. - Blood picture showed: a normal white blood cell count and normal erythrocyte sedimentation rate. Note: Drooping of upper eye lid may be in one or both eyes (ptosis).
Thank You Myasthenia Gravis Ptosis: Drooping of the upper eye lid of one eye
Questions about Myasthenia Gravis 1. Underline the symptoms of this patient and high lighten the signs mentioned in this case. 2. Based on your knowledge. Can you explain the symptoms & signs? 3. What do you think about the required investigations? 4. What is your (differential) diagnosis? 5. Can you suggest the lines of treatment of this patient?
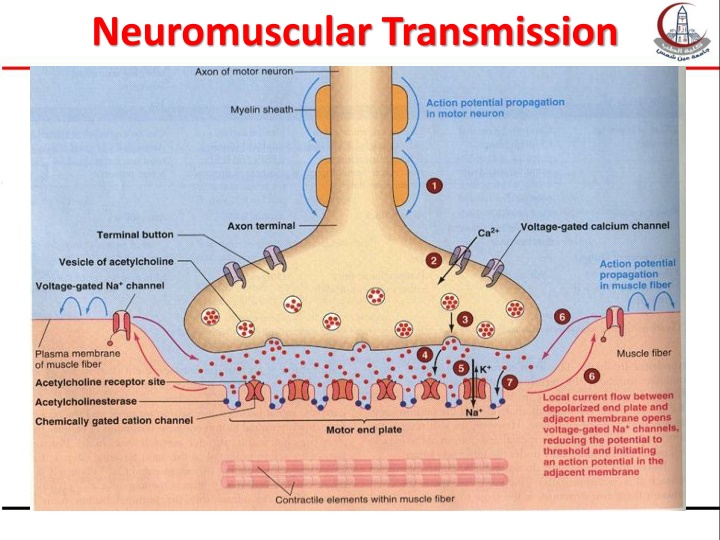
Causes of myasthenia: Autoimmune disease: antibodies against acetyl choline receptors or a protein called muscle specific receptor tyrosine kinase
Remarks With repetitive stimulation, decreased Ach release (depletion), together with diminished number of receptors cause declined transmission. This is the cause of the major symptom (fatigue with sustained activity)
Complications: Myasthenia Gravis crisis: When it affect respiratory muscle can lead to suffocation & death
Investigations 1. Nerve conduction test: will detect abnormalities in neuromuscular transmission. 2. Electromyography: electrical stimulation of the muscle will be normal 3. Pulmonary function tests: to exclude respiratory causes 4. Lab investigations: immunologic studies : serologic tests to detect the presence of Anti-AChR antibodies (+ve in 90% of myasthenic patients)
Differential Diagnosis Botulism Other myopathies: (differentiated by history, electromyography and muscle biopsy)
What is the treatment of this patient? 1) short acting anticholnesterase (neostigmine) ( each dose lasts 3-6 hours) 2) Immunosuppressive drugs (takes weeks to bring about effect) 3) Usually combined therapy ( 1 & 2) 4) corticosteroids 5) Plasmapheresis: which is plasma separation and removal of antibodies (short lived i.e. ends in weeks): is usually done in severe cases (myasthenic crisis i.e. respiratory muscle affection and possibility of suffocation and death)
A Case of Botulism Two patients, a married couple, presented at the hospital. Both complained of a dry mouth and swallowing difficulties, newly developed blurred vision, inability to sweat, urinary and stool retention, dizziness, and nausea. The severity of the symptoms differed among both patients and was less pronounced in the wife. The couple gave history of eating canned food the day before.
Categories of Botulism Foodborne botulism caused by eating foods that contain botulism toxin Intestinal botulism caused by ingesting spores of the bacteria which germinate and produce toxin in the intestines Wound botulism Clostridium botulinum spores germinate in the wound Inhalation botulism Aerosolized toxin is inhaled does not occur naturally and may be indicative of bioterrorism (use as a biological weapon)
Botulism Transmission Home-canned goods (foodborne) Honey (ingestion) can contain C. botulinum spores Crush injuries (wound) Botulism cannot be transmitted person-to-person
Botulism Pathophysiology Botulin toxin enters bloodstream from mucosal surface or wound Binds to peripheral cholinergic nerve endings Inhibits release of acetylcholine, preventing muscles from contracting Symmetrical, descending paralysis occurs beginning with cranial nerves and progressing downward Can result in airway obstruction or paralysis of respiratory muscles Botulinum toxin is the strongest neurotoxin known.
Botulism Clinical Presentation Classic symptoms of botulism poisoning include: blurred/double vision muscle weakness drooping eyelids slurred speech difficulty in swallowing patient is afebrile and alert
Botulism Clinical Treatment Antitoxin administration Effective in the treatment of foodborne, intestinal, and wound botulism Effectiveness for inhalation botulism has not been proven Supportive Care mechanical ventilation Administration of drugs to promote acetyl choline release parenteral nutrition Elimination Induced vomiting High enemas