Understanding Ovarian Reserve and Infertility Risks
Explore the concept of ovarian reserve and its impact on female fertility, including factors influencing oocyte quantity and quality, diminished ovarian reserve (DOR), and the importance of ovarian reserve testing in identifying infertility risks. Learn how ovarian reserve testing can provide crucial information for treatment planning and counseling in assisted reproductive technologies (ART).

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Ovarian reserve testing Ovarian reserve testing
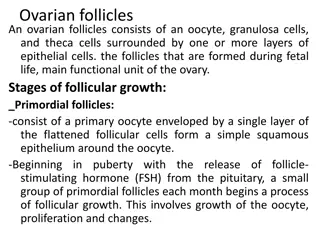
Oocytes Oocytes decrease in quantity and quality and do not regenerate Oocytes peaks at 6 7 million at fetal life (midgestation) 1 2 million oocytes at birth 300,000 500,000 at puberty, 1,000 at 51 years of age
Factors influence the quantity and Factors influence the quantity and quality of a woman s oocytes quality of a woman s oocytes Genetics Lifestyle Environment Medical issues Endometriosis ovarian surgery Chemotherapy and radiation
What is ovarian reserve ? What is ovarian reserve ? Ovarian reserve : a function of the number and quality of remaining oocytes Women of the same age have very different responses to ovarian stimulation Female fertility declines with age difficult to predict
What is ovarian reserve ? What is ovarian reserve ? Decreased or diminished ovarian reserve (DOR) Women of reproductive age having regular menses whose response to ovarian stimulation or fecundity is reduced compared with women of comparable age Usually defined as fewer than 3 5 developing follicles during an IVF cycle
DOR DOR In most cases, the cause(s) of DOR are unknown DOR resulting from Abnormally rapid atresia in a normal pool of oocytes From normal atresia of an abnormally small initial pool of oocytes Simply the extreme end of a normal bell-shaped population distribution of oocytes at a given age.
Ovarian reserve testing Ovarian reserve testing Goal To identify infertility patients at risk for DOR poor response to gonadotropin stimulation have a lesser chance of achieving pregnancy with ART Add more prognostic information to the counseling and planning process so as to help couples choose among treatment options.
Screening test Screening test Reproducible with low intercycle and intracycle variability Demonstrate high specificity to minimize the risk of a false-positive determination of decreased ovarian reserve in a woman with normal ovarian reserve
Who? Who? Ovarian reserve testing should be performed for Women > 35 years who have not conceived after 6 months of attempting pregnancy Women at higher risk of diminished ovarian reserve such as Hx of cancer treatment with chemotherapy,pelvic irradiation Medical conditions who were treated with gonadotoxic therapies Ovarian surgery for endometriomas
Ovarian reserve test Ovarian reserve test Ovarian reserve tests include Biochemical tests Ultrasound imaging of the ovaries
Ultrasound imaging of the ovaries Ultrasonographic measures of ovarian reserve Antral follicle count (AFC) Ovarian volume
Antral Antral Follicle Count Follicle Count Number of visible ovarian follicles measuring 2 10 mm in mean diameter in the greatest two-dimensional observed during transvaginal ultrasonography in the early follicular phase (cycle days 2 5) Low AFC considered 3 6 total antral follicles Meta-analysis, a low AFC was a mean of 5.2 Low AFC associated with Poor response to ovarian stimulation during IVF Not predict failure to conceive
Ovarian Volume Ovarian Volume Ovarian volume requires ovarian measurements in 3 planes and the use of the formula D1 D2 D3 0.52 Some ultrasound software may calculate automatically Mean ovarian volume: average volume calculated for both ovaries from the same individual Ovarian volume has limited value compared with AFC for detection of diminished ovarian reserve
Biochemical tests Biochemical tests Biochemical measures of ovarian reserve are intended to probe and to reflect the biology of the aging ovary Biochemical tests divided further into Basal measurements,including measurement of follicle-stimulating hormone(FSH) Estradiol inhibin B antimullerian hormone(AMH) Provocative tests clomiphene citrate challenge test (CCCT).
Basal Follicle-Stimulating Hormone FSH is released by the pituitary gland in response to gonadotropin- releasing hormone from the hypothalamus Subject to central negative feedback from estradiol and inhibin B. Novarian function, a developing follicles secretes estradiol and inhibin B suppress FSH, keeping it in the normal range. smaller follicular decreased estradiol , inhibin B levels increase in pituitary FSH secretion occurs, identified as an elevated early follicular phase FSH level. FSH level stimulates rapid ovarian follicular growth higher estradiol levels as well as a shorter follicular phase and reproductive cycle.
Basal Follicle-Stimulating Hormone Basal Follicle-Stimulating Hormone Advancing reproductive age, basal FSH increase on days 2 4 of the menstrual cycle High values of basal FSH (>10 20 IU/L) are associated with diminished ovarian reserve and poor response to ovarian stimulation A single elevated FSH value in women < 40 years predicts a lower oocyte yield during IVF but does not affect the rate of pregnancy
Basal Estradiol Estradiol is released from the ovary during follicular development. Estradiol level is usually low (<50 pg/mL) on days 2 4 of the menstrual cycle but demonstrates some cycle-to-cycle variability E2 (> 60 80 pg/mL) in the early follicular phase can indicate reproductive aging and hastened oocyte development High estradiol level can suppress an elevated FSH concentration into the normal range, estradiol level correct interpretation of a normal basal FSH level. Basal estradiol has low predictive accuracy for poor ovarian response and failure to conceive This test should not be used in isolation to assess ovarian reserve
Antimllerian Hormone AMH is a glycoprotein hormone produced by the granulosa cells of primary, preantral and antral follicles 2 6 mm in diameter reflects the size of the primordial oocyte pool Because early follicles secrete AMH in a gonadotropin independent state, AMH concentration is fairly stable within and between menstrual cycles
Antimllerian Hormone Age-related oocyte depletion decreae AMH levels Undetectable AMH level suggests diminished ovarian reserve and can identify individuals at risk of poor ovarian response to stimulation Undetectable and low AMH levels (0.2 0.7 ng/mL DSL ELISA) are not predictive of failure to conceive
Antimllerian Hormone AMH levels may allow treatment to be tailored to each individual. AMH is a good predictor of oocyte quantity, it may not provide information about quality. Young women with low AMH levels may have a reduced number of oocytes but normal,age-appropriate oocyte quality
Antimllerian Hormone limitation of AMH testing is the variability of results between the available assays and the inability to compare AMH levels when different assays are used. In clinical practice, individual AMH level test results must be interpreted based on the normal range of the assay used, and standard cutpoints may differ based on the assay AMH testing is a useful screening test in women at high risk of diminished ovarian reserve women undergoing IVF AMH limited benefits in women low risk of diminished ovarian reserve
Inhibin B Inhibin B is a glycoprotein hormone that is secreted primarily by preantral and antral follicles. The serum concentration of inhibin B decreases with the age-related decrease in the number of oocytes. Inhibin B has central negative feedback that controls FSH secretion; therefore a decrease in inhibin B levels leads to increased pituitary FSH secretion and higher early follicular FSH levels. However, there is significant variability in inhibin B levels between menstrual cycles. This marker does not reliably predict a poor response to ovarian stimulation and, thus, is not a recommended test
Clomiphene Citrate Challenge Test Method Measuring serum FSH on cycle day 3 Administering 100-mg clomiphene citrate daily on cycle days 5 9 Measuring serum FSH on cycle day 10. In women with a reduced number of ovarian follicles, lower E2 and inhibin B production leads to less central negative feedback of FSH secretion elevated FSH level after clomiphene stimulation
Limitation of CCCT : cycle to- cycle variability in ovarian biomarkers (ie, estradiol,inhibin B, and FSH) Elevated FSH level on cycle day 10 CCCT is predictive of poor ovarian response but is not predictive of failure to conceive
Ovarian reserve test For general obstetrician gynecologists The most appropriate ovarian reserve screening tests to use in practice are Basal FSH plus estradiol levels Antim llerian hormone (AMH) levels. An antral follicle count (AFC) useful if there is an indication to perform transvaginal ultrasonography