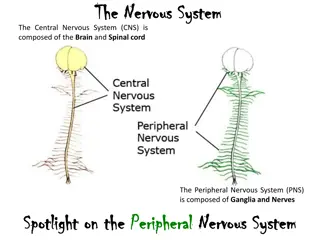
Understanding the Health System and Health Care Delivery
Explore the definition, objectives, and structure of the health system in Egypt, including the roles of the government, semi-governmental, and private sectors. Delve into the levels of health care delivery and the importance of primary health care in promoting community well-being.

Uploaded on | 0 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
The Health System Dr. Omnia Kamal Lecturer of public health and preventive medicine Faculty of Medicine, Minia University
Definition: A health system consists of all organizations, institutions, resources and people whose primary intent is to promote, restore or maintain health. A system is composed of discrete and interdependent compounds (subjects, objects, concepts) designed to achieve the goals.
Objectives of health system: 1- Universal health coverage 2- Achieving health goals and targets: Millennium Development Goals (MDGs) and Sustainable Development Goals (SDGS). Health services in Egypt are currently managed, financed, and provided by agencies in all three sectors of the economy: government, parastatal (semi -governmental), and private.
The government sector (MOHP) 1-manages the PHC centers and units, general hospitals, district hospitals, and integrated hospitals. 2- The governmental sector is composed of quasi-governmental organizations in which MOHP has a controlling share of decision making, and it includes the Health Insurance Organization, the Curative Care Organization, and the Teaching Hospitals and Institutes Organization. 3-Although a distinction is made between the government sector and the semi-governmental sector in describing the Egyptian health sector, both sectors are run by the state. The private sector Includes for-profit and nonprofit organizations and covers private pharmacies, private doctors, and private clinics and hospitals of all sizes
The health-care delivery system provides different types of health care (preventive and curative) at three levels: primary, secondary, and tertiary. 1-The MOHP provides about 40 percent of the health services delivered to the community. 2- The Health Insurance Organization provides care to governmental employees, school children, and neonates. About 50 percent of the population is covered by the health insurance system. 3- University, teaching, and research institutions provide 10 percent of health care. 4- The private sector provides about 12 percent of health services. 5-Health-care services may overlap, and an individual can receive services from more than one health-care sector.
Levels of Health Care A- Primary health care 1-The PHC is the first point of contact between the community and the health-care sector. 2-It covers almost 80% of the community needs. 3- Health services are provided by general practitioners (new graduates) through urban and rural health facilities. 4- The PHC is cost effective and is the least expensive level of health care.
B-Secondary health care 1- Secondary health care provides a higher level of curative care than PHC. 2- It covers 15% of the community needs. 3- Health services are provided by specialists in general and district hospitals and polyclinics. 4- A referral system exists between primary care and secondary care facilities. 5- Feedback of information and follow-up are essential elements of the referral system. 6- Secondary level of care is more costly.
C- Tertiary health care 1- Tertiary health care provides an advanced level of health-care and technology 2- through specialized hospitals and institutions and distinguished health-care specialists. 3- It covers 5% of the community health needs. 4- Tertiary level of care is expensive.
There are no formal referral systems in the MOHP delivery system. The MOHP service delivery units are organized along a number of different dimensions. These include geographic (rural and urban), structural (health units, health centers, and hospitals), functional (maternal child health centers), or programmatic (immunization, and diarrheal disease control). Health systems are made up of a horizontal system of general services, providing prevention and care for prevailing health problems, and of vertical programs for specific health conditions. Vertical programs are found more frequently where poverty prevails and epidemics flourish; general health services are weakly developed under such conditions
A- Horizontal Programs Focused on providing integrated health care for interrelated health problems for entire population and is usually financed by national health system. It is a basic unit for preventive and primary health care of national health system.
Advantages: 1- Sustainable - staff and facilities already in place in most countries 2- Greater possibility of patient and family-centered care over spectrum of life-cycle and health problems 3- Integrated management of multiple determinants of health nutrition, control of infection, preventive activities, health education, public health measures 4- Centralized medical records and information 5- Efficient use of scarce funding and resources Disadvantages: 1- Primary health care system weak in many countries (- Poorly funded -Health workers poorly trained for scope of work - Inconstant supply of medications and supplies) 2- May develop deficiencies in some health interventions 3- Difficult to document health outcomes poor accountability 4- Health care workers overwhelmed with multitude of interventions
B-Vertical programs The Ministry of health has attempted to target many health priorities in Egypt through vertical programs that rely heavily on donor assistance. Advantages: 1- Targeted resources to specific high priority health issues 2- Defined goals and objectives, with measurable outcomes high accountability 3- Often very successful in limited timeframe (smallpox eradication, malaria, immunization programs- esp. polio, onchocerchiasis, child health, HIV/AIDS) 4- Develop a sound evidence base for interventions 5- Good return on investment for donors
Disadvantages: 1- Weaken local health infrastructure, especially primary care Competition for health care staff focused programs pay more (up to 300%) and greater prestige Complex, multiple reporting structures and requirements Vertical program infrastructure not available for local, broader use (ie, HIV/AIDS treatment centers) 2- Fragmented health care, limited communication between programs and local health centers 3- Competition for limited funding among various vertical programs pressure to continue program regardless of outcomes and benefits 4- Lack of sustainability and up-scaling benefits and outcomes limited to target area and funding cycle.
PRIMARY HEALTH CARE PRIMARY HEALTH CARE AND AND QUALITY ASSURANCE PROGRAM QUALITY ASSURANCE PROGRAM
Alma Ata Declaration (1978) An international conference in Alma Ata issued a declaration which stated that Primary Health Care is the key to attain health for all (HFA)
Primary Health Care (PHC) It is the first level of contact of individuals, the family and community with the national health system bringing health care as close as possible to where people live and work, and constitutes the first element of a continuing health care process."
The concept of primary health care The concept of primary health care Essential health care: is the health care which would meet actual health needs of the community. Acceptable methods: accepted by all people Affordable health care: Affordability means PHC services are to be provided within the available resources Accessible health care (geographical- social)
Elements of PHC Elements of PHC There are eight elements of PHC. 1. Promotive services: 1.1. Education concerning prevailing health problems and the methods of preventing and controlling them 1.2. Promotion of food supply and proper nutrition. 1.3. Provision of comprehensive maternal and child health care.
. 2. Preventive services: 2.1. Immunization of children against major communicable diseases. 2.2. Prevention and control of locally endemic diseases. 2.3. Provision of adequate supply of safe water and basic sanitation. 3. Curative care: 3.1. Appropriate treatment of common diseases and injuries. 3.2. Provision of essential drugs.
QUALITY ASSURANCE PROGRAM IN PRIMARY HEALTH CARE Definition 1. Improving the quality of care in order to improve the health status of the community. 2. Ensuring appropriateness of the effective heath activities. 3.Maintaining predetermined standards of care for the health services provided for all members of the community when required.
Objectives of Quality Assurance Program 1- To set standards for the different activities and services provided by the health centers includes the eight elements of the PHC program.
2- To define sensitive and objective indicators for the assessment and the continuous monitoring of: a. Compliance with the preset standards. b. Outcome measures of health service activities & their impact on the community 3- To refine the processes of planning , monitoring and evaluation of PHC service.
What is the relationship between quantity and quality of health care? There is a strong positive association between the amount of resources dedicated to a health service and the quality of this service. This association continues to be true until it reaches a certain limit after which this positive association decrease as follows; a. When the allocated resources for health sector are limited the health facilities and services would be limited and as a result the quality is expected to be sub- optimal. b. Alternatively when the allocated resources for a health program are abundant, the quality gain could be disproportional to the cost
Elements: These represent the component parts that together form an activity . If an activity (e.g. immunization) is represented by a building thus the stones can be considered the elements that constitute this building. Similarly, the elements of immunization activity could include; refrigerator, thermometer, temperature chart of the refrigerator, syringes, immunization schedule, records, vaccines, recording, immunization techniques etc..
Criteria: As the elements constituting each activity are numerous, it is desirable to select elements that are precise, clear, effective, measurable and able to reflect the quality of that activity.
Standards: When the criterion has been defined at a descriptive or numerical level, it is referred to as standard. The standards can be described as ideal, optimal, reasonable. Defining a level for the criterion means, for example, the temperature of the refrigerator in the immunization room- should not exceed +8oC or a pregnant lady should make say 8 visits to the health staff supervising
The standards should be : - Comprehensive - Scientific - Practical - Relevant - Efficacious - Efficient - Feasible
Are standards subject to change ? Any set of standards for specific for specific health activity will require regular review to identify the need for ; - Modification, - Deletion, or - Substitution This review process should take place at agreed fixed periods of time, say up to five years, or following new developments in medical, health or pharmaceutical systems that might necessitate such changes.
Quality from the community view point means: a . A service that is available all the time b. Easily accessible c. Feeling of comfort d. Politeness of health providers. e. Disappearance of symptoms
Quality is perceived by the health care provider as: a . Technical skills b. Availability of resources and structure c. Freedom in health provision d. Achieving the target outcome For the health services owner quality means: a. Best services b. With least possible cost, and c. Achieving best outcome.
THE FRAMEWORK OF QUALITY ASSURANCE IN PHC 1. Structure. 2. Processes. 3. Outcome.
Measurement of the Quality of Structure Many experts in the filed of quality believe that good structure is the most important factor to assure care. However, the structure is considered an inaccurate service. This means that the characteristics of structure may only reflect the capacity to perform, however, the causative association between the structure and performance remains weak.
Processes / Procedures Donabedian defines the processes of health care as those huge and complex activities and reactions between doctors and patients. but, at the level of Primary Health Care, we consider community as one of the most important elements in the PHC program. The processes- involve: 1. All health team members (doctors, nurses, health inspector s social workers, 2. All community members (health and diseased of all age categories of both sexes.) 3. All health related sectors (municipality, education, agriculture , etc. ) 4. The inter- relationship team members.
Measuring the Quality of Process The data concerning the quality of process can be obtained by either direct observation or reviewing records, files or reports. Also, this can be achieved by direct interview with the catchment area. In general, measurement of a process quality depends on the nature of the process itself.
Outcome/ Results These words refer to the change(s) that is (are) observed in the individual, community or environmental health. In general, it is the change required by the health program. Measuring the Quality of Outcome The outcome of disease, for example, can be classified for simplicity into what is referred to as the five Ds : - Death - Disease - Disability - Distress - Dissatisfaction However, the morbidity and mortality rates remain the most important and easiest tools to measure the quality of most health services.
N.B. While Measuring the Outcome: Changes in outcome often occur after the implementation of changes in structure and or process. Improvement in quality of may be dependent on better utilization of available resources (process) rather resources (structure).
ASSESSMENT OF THE QUALITY OF HEALTH SERVICES Assessment has to try to answer this question: What happened? In the context of quality assurance, assessment answers the following question: Have we done what we said we would? Or in other words: Do we have defined standards against which we are going to assess? To answer this question, five steps should be followed 1. Collection of data 2. Analysis of trends 3. Interpretation of results 4. Corrective actions 5. Follow-up
Community participation Community participation Community is defined as a group of people with diverse characteristics who are linked by social ties, share common perspectives, and engage in joint action in geographical locations or settings. The community should play an important role in the implementation of health services based on their needs and awareness. Generally, people are ready and willing to participate.
WHO defined community participation as a process by which people are enabled to become actively and genuinely involved in: - Defining issues of concern to them - Making decision about factors that affect their life - Formulating and implementing policies in planning, developing and delivering services - Taking action to achieve change
Definition of Community participation is the process by which individuals and families mobilize its resources, initiate and take responsibility for their own health and welfare, and share in decision making and develop the capacity to contribute in implementation of community's development. They come to know their own situation better and are motivated to solve their common problems. This enables them to become agents of their own development instead of passive beneficiaries of development aid.
Aims of community participation: - The community develops self-reliance - The community develops critical awareness - The community develops problem solving skills - Contributes towards feeling of responsibility and accountability - Save time and resources
Levels of participation: 1- Passive participation: People participate by being told what is going to happen or has already happened through unilateral announcement by administration. 2- Active participation: carrying out some tasks in a program but are not involved with the final decision making Ex: They could share in the delivery of services to the people as volunteers in activities such as house campaigns of Polio vaccination throughout the whole Egypt; and the participation of local leaders in health education. 3- Involvement (Community control): involving the community in planning, implementation, management and evaluation of programs i.e. people's health in people's hands.
Steps of community participation process: 1- Situation analysis in local community 2- Establishment of the Community Design Team (CDT) 3- Review of data 4- Identify priority needs and audience 5- Define and understand the target audience 6- Develop educational and behavioral objectives
7- Develop messages and strategies 8- Construct program plan 9- Implement plan To achieve community participation, put in consideration: 1- Make the community self-sufficient through its own initiatives and resources or with a minimum outside assistance. 2-Considering the prevailing situation. 3- Respecting that changes are slow and that traditions are strong



")












")