Understanding Trauma: Types, Treatment Principles, and Interventions
Explore the complexities of trauma, from different types to evidence-based treatment principles. Learn about trauma stages, eco-social interventions, and the impact on individuals. Discover how trauma manifests and the importance of safety and connection in the recovery process.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
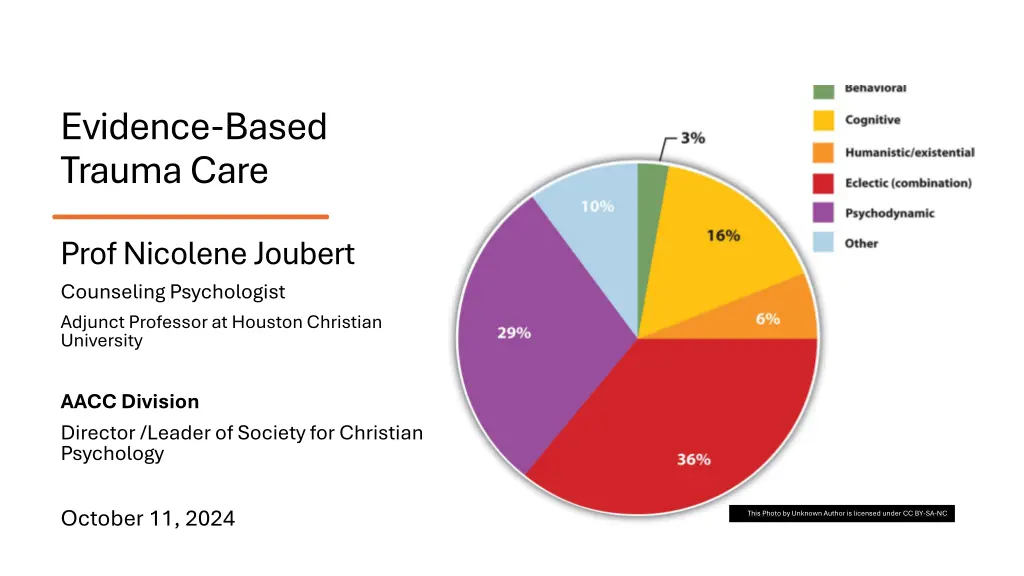
Evidence-Based Trauma Care Prof Nicolene Joubert Counseling Psychologist Adjunct Professor at Houston Christian University AACC Division Director /Leader of Society for Christian Psychology October 11, 2024 This Photo by Unknown Author is licensed under CC BY-SA-NC
Learning Objectives Explain and describe the central treatment principles and stages of trauma and recovery (Briere & Scott, 2014) Stage 1:Provide and Ensure Safety Maintain a Positive and Consistent Therapeutic Relationship Stage 2: Tailor the therapy to the client Take gender issues into account Monitor and control counteractivation/ countertransference Practice ethically within the standard of care Stage 3:Reconnection Stage 4: Meaning-making and Post-traumatic Growth Compare and contrast evidence-based trauma care Prolonged Exposure ( for PTSD) (includes imaginal exposure to the trauma) Cognitive Processing Cognitive Behavioral therapy Narrative Exposure therapy (NET) (this approach also includes the lifeline) Explain and Demonstrate a Christian Narrative Approach
Eco-Social Trauma Intervention Model Transdisciplinary approach Cultural and collective trauma Going beyond Western paradigm of treating trauma through individual psychotherapy/counseling
What is trauma? Trauma is a complex phenomenon that encompasses Range of experiences, Natural disasters and accidents Interpersonal violence and childhood abuse Overwhelm individual's capacity to cope Leading to profound psychological distress and Disruption in daily functioning Trauma can manifest in various ways, including Intrusive thoughts, Emotional numbness Hypervigilance, and Avoidance behaviors
Types of trauma Acute : single, short event Chronic : persistent or ongoing Complex: complex combination of events interpersonal or childhood abuse Development trauma : trauma occur during certain developmental periods Systemic: historical, political, socio-economic events
Three Stages Based on the work of Herman (2022) Stage 1 Safety, stabilization and symptom management Stage 2: Implement therapy model Prolonged Exposure ( for PTSD) (includes imaginal exposure to the trauma) Cognitive Processing Cognitive Behavioral therapy Narrative Exposure therapy (NET) (this approach also includes the lifeline) Stage 3: Reconnection
What is trauma? Trauma refers to the emotional and psychological and physical responses that occur when individuals are exposed to events or circumstances that are either life threatening or perceived as such Trauma syndromes are complex Cultural and collective trauma whole communities Treatment must be comprehensive Eco-social and systemic approach
Types of Trauma Natural disasters (tsunami, bush fires, tornados and storms) Acts of violence (war, violent conflict, armed robbery, murder) Accidents (car, fire) Personal losses (death of a loved one, job loss, divorce) Chronic or systemic stressors (living in poverty, persecution, discrimination, acculturative stress) Political changes and movements
Individual Responses to Trauma Differ from person to person depending on past experiences, resilience, support groups Psychological impact Physical effect Social impact Spiritual impact
Trauma recovery: The Healing Relationship The core of psychological trauma is disempowerment and disconnection Second principle: restore control Survivors feel unsafe in their bodies Feel unsafe in relation to other people Recovery has to take place in the context of relationships First principle: the empowerment of the survivor Interventions should not take power away It cannot take place in isolation
Therapist/client is a unique relationship Traumatic Transference Healing Relationship Traumatic Countertransference Therapy Contract Therapist Support System
Therapist/client relationship Quality of congruence, genuineness and acceptance Ability reflect is essential for effective healing process Reflect on transference and countertransference dynamics Identify transference and countertransference emotions and behavior
Traumatic Transference Intense, life-or-death quality Unparalleled in ordinary therapeutic experience Patient has to keep therapist under control Violence of perpetrator may be expressed towards therapist Terror is as though patient and therapist convene in presence of another person the perpetrator who demanded silence Reflect powerlessness of patient Complex trauma Complex transference issues Reference Herman, J. L. (2015). Trauma and Recovery. Hachette. https://bookshelf.vitalsource.com/books/9780465098736
Traumatic countertransference vicarious trauma Therapist experiences symptoms of post-traumatic stress disorder Patient s trauma story revives personal traumatic experiences Therapist have suffered in the past Imagery associated with the patient s story intruding own waking fantasies or dream Nightmares Entire range of emotions to the survivor and trauma itself Therapist may underestimate the value of her own knowledge and skill Violating bounds of time limits and give more time to survivor Therapist defense against stance of helplessness - grandiose thinking see herself as the rescuer Experience anger and rage, grief or other emotions identification with the patient Lead to more disempowerment of patient Therapist experience confusion of inner conflict in abused child Bystanders to trauma suffers witness guilt Reference Herman, J. L. (2015). Trauma and Recovery. Hachette. https://bookshelf.vitalsource.com/books/9780465098736
Therapy contract Both parties are responsible for the relationship Fundamental rule is to commit to telling the truth Explain process Be prepared to repeat testing, disruption and rebuilding of the relationship Explain confidentiality and limits Explain boundaries Therapy relationship precludes any other social relationship Discuss expectations and goals Financial obligations
Therapists own support system Threat for the psychological health of the therapist Needs a support system Supervisor or mentor Church/prayer group can be helpful, but confidentiality cannot be broken Colleagues
Three Broad Stages of Recovery (Herman, 2015) (Briere and Scott, 2014) Syndrome Hysteria first emergence of trauma Combat Trauma Stage 1 Stabilization symptom orientation Stage 2/ Stage 3 & 4 Exploration of traumatic memories Stage 3/4 Personality reintegration, rehabilitation Trust, stress management, education Stabilization Reexperiencing memories Integration of trauma Complex PTSD Integration of memories Development of self, drive integration Resolution, integration, development of post- integration skills Reconnection Multiple Personality Disorder (DID) Diagnosis, stabilization, cooperation, communication Impact of trauma on metabolism Traumatic Disorders Safety Remembrance and Mourning
Stage 1: Stabilization and Safety Safety starts with the body Medical examination and attention to injuries Control of the body focuses on restoration Safe environment Finding and securing refuge Relationships with other will oscillate surround with people or isolate Families and friends lives will be disrupted Support system needs to be created Criminal reporting rests with the client Self care is disrupted and may take several forms Suicidality Self mutilation Eating disorders
Safety and self care Patient is encouraged to draw up a plan for safety She has to build capacities and exercise control Attempts may be sabotaged Encouragement should be consistent from therapist Single most common error in therapy Avoiding the content of the traumatic event(s) Second most common error Encouraging the telling of the story in graphic details prematurely There is no quick and magical cure through catharsis Completing the first stage: client is confident in her abilities to practice self care and protect herself
Stages 2, 3 & 4: Remembrance and Mourning (Herman, 2015) (Briere & Scott, 2014) During this stage the survivor tells the story Completely, in depth, in detail The work of reconstruction transforms the story The event can be integrated into the survivor s life story Initially the story may be repeated, Does not develop or progress in time Does not reveal emotions or interpretation of events During this time the need for safety must be balanced with the trauma being relived
Traumatic narrative needs to have trauma imagery Bodily sensations Goal is to put the story into words Remembrance and Mourning Questions to ask - what is the person seeing, hearing, smelling, touching Facts have to be reconstructed but what the survivor experienced (feelings, thoughts, etc.) A sense of meaning has to be constructed
Stage 3 & 4: Meaning-making & Post-traumatic Growth (Briere, 2014) Compare and contrast evidence-based trauma care Prolonged Exposure ( for PTSD) (includes imaginal exposure to the trauma) Cognitive Processing Cognitive Behavioral therapy Narrative Exposure therapy (NET) (this approach also includes the lifeline)
Prolonged Exposure for PTSD (endorsed by the Institute of Medicine) as sufficiently evidenced-based Pavlovian concept of conditioning Stage 3 & 4 Transforming Traumatic Memory Exposure to stimulus associated with trauma in safe environment Deconditioned The impact of trauma is far more complex than what a fear conditioning model can explain Prolonged exposure client has to tell in detail for most horrific experiences can be harmful Stage 1 must be solid
Cognitive processing Two major ways for cognitive processing Describing them in detail In as much detail as tolerable include feelings Feelings are important for emotional processing Discussion of conclusions or beliefs that a client has formed Open-ended questions aimed at making the cognitive distortions clear Writing about them Bring writings to the session and read out loud Mere act of writing, done on multiple occasions, can reduce psychological distress Actively activate traumatic memories and process during consequent discussions Socrative dialogue gentle inquiries to help a client examine assumptions Client is encouraged to explore distorted beliefs, self-blame, guilt Develop a coherent narrative Cognitive reconsideration can lead to insight
Cognitive Behavioral Therapy Individuals who have experienced trauma often develop cognitive distortions, or Irrational beliefs and thought patterns, that contribute to their distress and dysfunction. Common cognitive distortions in trauma include: Catastrophizing Personalization All-or-nothing thinking Overgeneralizing
Principles Psycho-education Educate about trauma Skills building Work with client s strengths and build new skills Gradual exposure Remembrance of event retelling the story Cognitive restructuring Address cognitive distortions Safety and trust Provide safe environment
Narrative Exposure Therapy Narrative Exposure Therapy (NET) is a short-term psychotherapy Treatment of post-traumatic stress disorder and trauma-related mental disorders NET combines cognitive restructuring, story production, and exposure treatment. The theory is based on the idea that people can become masters of their memories promote emotional healing by systematically reliving painful events in a therapeutic environment.
Comparison Comparison Prolonged exposure Cognitive Processing Cognitive-behavioral therapy Narrative Exposure Therapy Pavlov Conditioned behavior Exposure to trauma Cognitive processing Cognitive and behavioral aspects Verbal account Social-Interpersonal Theory Verbal account and emotional exposure Reconstruction of trauma Verbal and written accounts Focus/purpose of intervention Deconditioning of fear response Explore cognitive distortions Explore skills & Cognitive Distortions Restructure story Emotional healing Techniques Retelling of story in detail Detailed account Read written work Socratic method Imaginal exposure In-vivo exposure triggers in real life Relaxation Emotional regulation Safe therapeutic relationship Collaboration Cultural consideration Coherent narrative Exposure Story production Systematically relive painful events Connections/ relationships Safe environment Therapeutic relationship Reconsider cognitive beliefs Connect to self & others Coherent narrative People can become the masters of their memories Therapeutic context Coherent narrative Meaning-making Post-Traumatic Growth Insight Future Growth and future focus Future focus
Group discussion: Questions Q 1 Discuss the benefits of each approach and gaps? Q2 What are central themes covered in all the approaches? Q3 What is the most important goal in trauma counseling? Q 4 How could you prevent early dropouts? Q5 Which approach would you prefer? Why? Q 6 Critique on secular methods from Christian Worldview?
Feedback Feedback on group discussion
References Briere, J. N., & Scott, C. (2014). Principles of Trauma Therapy (2nd ed.). SAGE Publications, Inc. (US). https://bookshelf.vitalsource.com/books/9781483351254 Eftekhari, A., Crowley, J., Mackintosh, M., & Rosen, C. (2020). Predicting Treatment Dropout Among Veterans Receiving Prolonged Exposure Therapy. Psychological Trauma: Theory, Research, Practice, and Policy, 12(4), 405-412. Frank, H., Last, B., AlRabiah, R., Fishman, J., Rudd, B., Kratz, H., Harker, C., Fernandez-Marcote, S., Jackson, K., Comeau, C., Shoyinka, S., & Beidas, R. (2021). Understanding therapists perceived determinants of trauma narrative use. Implementation Science Communications, 2(1) Gingrich, H.D.G. C. (2017). Treating Trauma in Christian Counseling. InterVarsity Press. https://bookshelf.vitalsource.com/books/9780830889129 Herman, J. L. (2022). Trauma and Recovery. Hachette. https://bookshelf.vitalsource.com/books/9780465098736
References Lisa L pez Levers, PhD, LPCC-S, LPC, C. Trauma Counseling. Available from: VitalSource Bookshelf, (2nd Edition). Springer Publishing LLC, 2022. McLean, C., & Foa, E. (2024). State of the Science: Prolonged exposure therapy for the treatment of posttraumatic stress disorder. Journal of Traumatic Stress, 37(4), 535-550 Torres, P., Ignacio, D., & Gottlieb, M. (2023). Reducing the Cost of Caring: Indirect Trauma Exposure on Mental Health Providers. Journal of EMDR Practice and Research, 17(1), 2-11. M.D., Bessel van der K. The Body Keeps the Score. Available from: VitalSource Bookshelf, Penguin US, 2014. Wild, J., Warnock-Parkes, E., Murray, H., Kerr, A., Thew, G., Grey, N., Clark, D., & Ehlers, A. (2020). Treating posttraumatic stress disorder remotely with cognitive therapy for PTSD. European Journal of Psychotraumatology, 11(1), 1 Wood, M. (2017). Book Review: Leading with Story: Cultivating Christ- Centered Leaders in a Story-centric Generation. Missiology, 45(2), 217-217. Wright, H. N. (2011). The Complete Guide to Crisis & Trauma Counseling. Baker Publishing Group. https://bookshelf.vitalsource.com/books/9781441267580