Clinical Manifestations and Renal Syndromes Overview
Clinical manifestations of renal diseases such as azotemia and uremia, along with an overview of major renal syndromes like nephrotic syndrome. Learn about the pathogenesis and characteristics of these conditions.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
RENAL PATHOLOGY FOR DENTAL Fatima Obeidat, MD
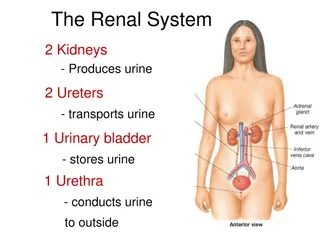
I. The clinical manifestations of renal diseases
A. Azotemia - Is an elevation of blood urea nitrogen and creatinine levels - Usually reflects a decreased glomerular filtration rate (GFR). - GFR may be decreased as a consequence of intrinsic renal disease or extrarenal causes. .
i. Prerenal azotemia is encountered when there is hypoperfusion of the kidneys, which decreases GFR in the absence of parenchymal damage ii. Postrenal azotemia results when urine flow is obstructed below the level of the kidney. - Relief of the obstruction is followed by correction of the azotemia
B Uremia - When azotemia gives rise to clinical manifestations and systemic biochemical abnormalities. - There is secondary gastrointestinal (e.g., uremic gastroenteritis);neuromuscular (e.g., peripheral neuropathy); and cardiovascular (e.g., uremic fibrinous pericarditis)
The major renal syndromes
I. Nephrotic syndrome -Is a glomerular syndrome characterized by: a. Massive proteinuria (excretion of greater than 3.5 g of protein/day in adults). b. Hypoalbuminemia, with plasma albumin levels less than 3 g/dL.
c. Severe edema d. Hyperlipidemia e. Lipiduria (lipid in the urine).
Pathogenesis - The causes of this syndrome result in derangement in the capillary walls of the glomeruli that results in increased permeability to plasma proteins.
- Any increased permeability resulting from either structural or physicochemical alterations in the GBM allows protein to escape from the plasma into the glomerular filtrate
- With long-standing or extremely heavy proteinuria,: a. Serum albumin is decreased, resulting in hypoalbuminemia b. A drop in plasma colloid osmotic pressure.
- The resulting decrease in intravascular volume and renal blood flow triggers increased release of renin from renal juxtaglomerular cells - Renin in turn stimulates the angiotensin- aldosterone axis, which promotes the retention of salt and water by the kidney.
- In the face of continuing proteinuria, these alterations further aggravate the edema and if unchecked may lead to the development of generalized edema (termed anasarca). - At the onset, there is little or no azotemia, hematuria, or hypertension.
- The relative frequencies of the several causes of the nephrotic syndrome vary according to age a. In children 1 to 7 years of age: The nephrotic syndrome is almost always caused by a lesion primary to the kidney
b. Among adults it often is due to renal manifestations of a systemic disease: - The most frequent systemic causes of the nephrotic syndrome in adults are i. Diabetes ii. Amyloidosis iii. Systemic lupus erythematosus.
- The most important of the primary glomerular lesions that characteristically lead to the nephrotic syndrome are: a. Minimal-change disease which is is more important in children b. Focal and segmental glomerulosclerosis which is more important in adults
Two other primary lesions, c. Membranous nephropathy d. Membrano-proliferative glomerulonephritis,.
I.Minimal-Change Disease - Is a relatively benign disorder - Is the most frequent cause of the nephrotic syndrome in children.
Pathology a. By light microscopy: The glomeruli have a normal appearance b. By electron microscope: The glomeruli show diffuse effacement of podocyte foot processes when
Clinically -The proteinuria is confined to the smaller plasma proteins, chiefly albumin (selective proteinuria). - The prognosis for children with this disorder is good
II. Focal segmental glomerulosclerosis (FSGS) - Histologically it is characterized By: i. sclerosis affecting some but not all glomeruli (focal involvement) ii. involving only segments of each affected glomerulus (segmental involvement).
Clinically - The associated proteinuria is nonselective - In general the response to corticosteroid therapy is poor. - The incidence of hematuria and hypertension is higher in persons with FSGS than in those with minimal-change disease.
Clinical Course -At least 50% of patients with FSGS develop end-stage kidney disease within 10 years of diagnosis. - Adults typically fare even less well than children
III. Membranous Nephropathy - Is a slowly progressive disease, - Most common between 30 and 60 years of age. - Histologically, the main feature is diffuse thickening of the capillary wall
Clinical Course - Most cases present as full blown nephrotic syndrome - The proteinuria is nonselective, with urinary loss of globulins as well as smaller albumin molecules - Does not usually respond to corticosteroid therapy
Clinical Course - Only about 40% suffer progressive disease terminating in renal failure after 2 to 20 years. - An additional 10% to 30% have a more benign course with partial or complete remission of proteinuria.
IV. Membranoproliferative Glomerulonephritis and dense Deposit Disease - It accounts for 5% to 10% of cases of idiopathic nephrotic syndrome in children and adults. - Two major types of MPGN a. Type I: Termed MPGN type I b. Dense deposit disease (formerly MPGN type II) - Of the two types of disease, MPGN type I is far more common
Clinically a. Some patients present only with hematuria or proteinuria in the non- nephrotic range b. Others exhibit a combined nephrotic nephritic picture-
The Nephritic Syndrome a. Is a clinical complex b. Usually of acute onset c. Characterized clinically by:
(1)hematuria with dysmorphic red cells and red cell casts in the urine; (2) some degree of oliguria (3)some degree of and azotemia; (4) hypertension. (5) although proteinuria and even edema also may be present, these usually are not as severe as in the nephrotic syndrome.
Pathogenesis - The lesions that cause the nephritic syndrome have in common: a. Proliferation of the cells within the glomeruli b. Often accompanied by an inflammatory leukocytic infiltrate
- This inflammatory reaction : a. severely injures the capillary walls, permitting blood to pass into the urine b. induces hemodynamic changes that lead to a reduction in the GFR.
- The reduced GFR is manifested clinically by a. Oliguria, b. Fluid retention c. Azotemia. d. Hypertension probably is a result of both the fluid retention and some augmented renin release from the ischemic kidneys .
- The acute nephritic syndrome may be produced by: a. systemic disorders such as systemic lupus erythematosus, b. or it may be secondary to primary glomerular disease. - The latter is exemplified by acute postinfectious glomerulo nephritis
Acute Postinfectious (Poststreptococcal) Glomerulonephritis - Is one ne of the more frequently occurring glomerular disorders, - is caused by glomerular deposition of immune complexes resulting in a. proliferation of and damage to glomerular cells and b. infiltration of leukocytes, especially neutrophils.
- The classic case of poststreptococcal GN develops in a child 1 to 4 weeks after they recover from a group A streptococcal infection. - Only certain nephritogenic strains of - hemolytic streptococci evoke glomerular disease.
Clinical Course - The onset of the kidney disease tends to be abrupt, heralded by a. Malaise, b. A slight fever and nausea. c. The nephritic syndrome.
Clinically - Characterized by a. gross hematuria and the urine appearing smoky brown rather than bright red In the usual case, b. oliguria, azotemia, and hypertension are only mild to moderate. c. Some degree of proteinuria is a constant feature of the disease,
- Serum antistreptolysin O antibody titers are elevated in poststreptoco- ccal cases. -.
- Recovery occurs in most children in epidemic cases - In adults, 15% to 50% of affected persons develop end-stage renal disease over the ensuing few years or 1 to 2 decades, depending on the clinical and histologic severity.
IgANephropathy - IgAnephropathy is one of the most common causes of recurrent microscopic or gross hematuria - And is the most common glomerular disease revealed by renal biopsy worldwide.





































hematuria with dysmorphic red cells and red")




")