Nephrotic Syndrome in Pediatrics: Overview and Insights
Discover the key aspects of nephrotic syndrome in pediatrics including its epidemiology, classification, etiology, pathophysiology, clinical features, investigations, treatment, complications, and prognosis. Understand the different types and causes of this syndrome along with the common age groups affected, prevalent symptoms, and potential complications for effective management.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Nephrotic Syndrome in Pediatrics Presenter: Kessy Julius P. Intern Dr . Supervisor: Christina K. Galabawa, MD, Mmed 2, Pediatrics and Child Health, UDOM. DODOMA REGIONAL REFERRAL HOSPITAL (DRRH)
Outline Introduction Epidemiology Classification & Etiology Pathophysiology Clinical features Investigations & treatment Complications & prognosis 1.
Introduction Syndrome caused by renal diseases that increase the permeability across the glomerular filtration barrier. Characterized by a tetrad of clinical features 2.
Contd 1. Nephrotic range proteinuria Urinary protein excretion > 50 mg/kg/day. 2. Hypoalbuminemia Serum albumin concentration < 3g/dl (30g/l). Hyperlipidemia Edema. 3. 4. 3.
Epidemiology Occurs at all ages but most prevalent in children 1.5-6 years. Boys > girls, 2:1 ratio. Higher in underdeveloped countries (South east Asia and Africa). Incidence worldwide, 2 7 cases per 100,000 children/year. 4.
Classification & Etiology 1. Primary No identifiable systemic disease. These are patients with; I. Idiopathic NS No glomerular inflammation on renal biopsy. II. Primary glomerulonephritis Active sediment and glomerular inflammation on biopsy. 5.
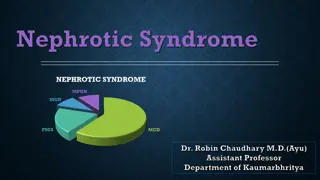
Contd 2. Idiopathic I. Minimal Change Disease (MCD) - 85% II. Focal Segmental Glomeruloscrelosis (FSGSS) III. Membranoproliferative glomerulonephritis IV. Mesangial proliferation V. Membranous nephropathy >80% of children with idiopathic NS are steroid sensitive. 6.
Contd 3. Secondary Infections Viral (HBV, HCV & HIV), Bacterial (Streptococcal) and parasites (Malaria). Others are syphilis and toxoplasmosis. Systemic conditions Autoimmune (SLE & vasculitis), Metabolic (Diabetes & amyloidosis), Malignancies (Leukemia & lymphomas), Hematological (SCA), Obesity. 7.
Contd Allergy bee sting, cow s milk, pollen, house dust. Drugs NSAIDs, Ampicillin, penicillamine, gold, captopril and lithium. 8.
Contd 4. Hereditary NS Below one year. 9.
Clinical features Periorbital puffiness: more marked in the morning and later generalized Scrotal edema Pleural effusion and Ascites are late features Decreased urine output Hypertension and hematuria are absent 10.
Clinical features . 11.
Clinical features . 12.
Clinical features . 13.
Clinical features . 14.
Investigations Urinalysis I. Proteinuria +3 or +4 II. Urinary protein excretion (>40mg/m2/hour) III. 24 hours urinary protein : creatinine > 3 IV. Microscopic hematuria in 10% V. Pus cells in underlying UTI VI. Cellular casts in other forms not MCD 15.
Contd Serum I. II. Others I. II. Albumin < 3g/dl Cholesterol > 250mg/dl CBC usually normal, raised ESR CXR to R/O pleural effusion 16.
Contd Renal biopsy (Indications) I. SRNS II. Frequent relapses III. Steroid toxicity IV. Secondary NS V. Gross hematuria VI. Hypertension VII. Renal insufficiency 17.
T reatment High dose steroids -2mg/kg (max 60) daily for 6 weeks -1.5mg/kg (max 40) alternating days for 6 weeks (If attained remission) Relapse management -Precipitated by minor infections -Treatment of infections often result in remission for +1-2 proteinuria 18.
T reatment Persistent +3-4 needs steroids -2mg/kg (max 60) daily until remission, then 1.5 mg/kg on A/D for 4 weeks. Steroid dependant and frequent relapses -Long term steroid therapy -0.3-0.7 mg/kg on A/D for 9-18 months. 19.
Special definitions Remission: trace/no protein in urine on dipstick for 3 consecutive days. Relapse: urine protein is 3+/4+ for three consecutive days after having attained remission. Frequent relapser: four or more relapses in 12 months. 20.
Special definitions Steroid dependent: two consecutive relapse while on A/D steroids or within 14 days of its discontinuation. Steroid resistant: proteinuria (+2 or more) on daily steroid therapy after 8 weeks. 21.
T reatment Supportive management: Diet - Adequate in proteins and calories - Fluid and salt restriction in edema Hospitalization -Infections -Marked edema - Monitoring BP in hypovolemia 22.
T reatment Diuretics -massive ascites, pleural effusion and severe genital edema Ambulation & Anti coagulants for thromboembolism ACEI in hypertension Calcium carbonate and vitamin D in Osteoporosis 23.
Complications Infections -SBP, Pneumonia, UTI -Sepsis -Cellulitis Arterial and Venous Thrombosis Steroids and other drugs adverse effects 24.
Prognosis Response time: 10% by the end of first week 70% by the end of second week 85% by the end of third week 92% by the end of fourth week 25.
Contd Steroid responders 90% Minimal change disease 50% Mesangial proliferation 20% Focal sclerosis 26.
Contd Poor prognostic factors -Hematuria -Hypertension -Hypocomplementemia -Focal segmental sclerosis -Steroid resistance 27.
THANK YOU!!! To study the phenomenon of disease without books is to sail an uncharted sea while to study books without patients is not to go to the sea at all - William Osler. 28.






























![❤[PDF]⚡ Zee Zee Does It Anyway!: A Story about down Syndrome and Determination](/thumb/20462/pdf-zee-zee-does-it-anyway-a-story-about-down-syndrome-and-determination.jpg)