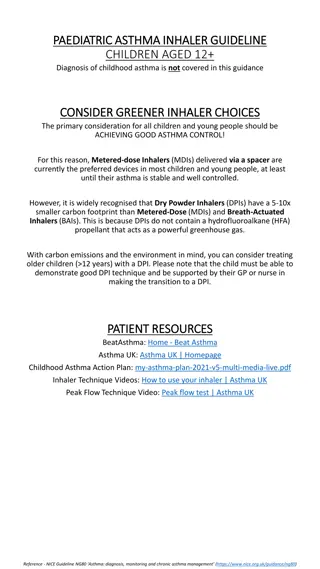
Risk Factors for Asthma Attacks in Adults
The risk factors associated with future asthma attacks can help healthcare providers in assessing and managing patients with asthma. Factors such as previous asthma attacks, poor control, age, gender, lung function, obesity, smoking, and depression play a role in determining the likelihood of future asthma exacerbations. Identifying these risk factors early on enables targeted interventions to prevent or reduce the frequency of asthma attacks.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Asthma SCE Qs Asthma SCE Qs Bea Downie Bea Downie
Q1. Q1. You see a 28yr old man in clinic for review of his chronic asthma. He has had 2 asthma attacks in the last year. PMHx: Asthma, Obesity, Fibromyalgia, Depression. He works as a secretary, lives alone and smokes 10/day. Spirometry reveals an obstructive picture with reversibility. In this patient, which of the following is not considered to be a marker of an increased risk of future asthma attacks? A) Previous asthma attacks B) Male gender C) Reduced lung function D) Obesity E) Smoking F) Depression
Q1. Q1. You see a 28yr old man in clinic for review of his chronic asthma. He has had 2 asthma attacks in the last year. PMHx: Asthma, Obesity, Fibromyalgia, Depression. He works as a secretary, lives alone and smokes 10/day. Spirometry reveals an obstructive picture with reversibility. In this patient, which of the following is not considered to be a marker of an increased risk of future asthma attacks? A) Previous asthma attacks B) Male gender C) Reduced lung function D) Obesity E) Smoking F) Depression
Factors associated with increased risk of future asthma attacks. Level of Increased Risk Factor Greatly Increased Risk History of previous asthma attacks. Moderately Increased Risk Poor control. Inappropriate or excessive SABA use. Slightly Increased Risk Older age. Female. Reduced lung function. Obesity. Smoking. Depression. Ref: BTS/SIGN Guideline for the Management of Asthma, July 2019, pg 33
Q2 A 45yr old asthmatic patient presents with 24hrs of breathlessness, wheeze and chest tightness. RR 26, Sats 93%, HR 115, BP 89/45. You note she is in AF. Her PEF is 150L/min. Her usual best PEF is 300L/min. Which two of the following are indications to perform an Arterial Blood Gas? A) Sats of 93% B) Arrhythmia C) PEF of 150L/min. D) Hypotension
Q2 A 45yr old asthmatic patient presents with 24hrs of breathlessness, wheeze and chest tightness. RR 26, Sats 93%, HR 115, BP 89/45. You note she is in AF. Her PEF is 150L/min. Her usual best PEF is 300L/min. Which two of the following are indications to perform an Arterial Blood Gas? "Patients with SpO <92% or other features of life- threatening asthma require ABG measurement." A) Sats of 93% B) Arrhythmia C) PEF of 150L/min. D) Hypotension BTS/SIGN Guideline for the Management of Asthma, July 2019
Patients with Patients with SpO life life- -threatening asthma threatening asthma require ABG measurement. require ABG measurement. SpO <92% or other features of <92% or other features of
Q3 Q3 You see a 35yr old pregnant woman in asthma clinic. She asks if there is any special advice for managing asthma in pregnancy/labour. Regarding asthma in pregnancy, which of the following is false false....? A) If anaesthesia is required, regional blockade is preferred to GA due to the risk of some inhaled anaesthetic agents causing bronchospasm. C) Prostaglandin F2 should be used with extreme caution in women with asthma because of the risk of inducing bronchoconstriction. D) Continuous fetal monitoring is recommended for women presenting with acute severe asthma whilst pregnant. E) Those taking > 5 mg/day of prednisolone for >2 weeks prior to delivery should receive hydrocortisone 100 mg IV 6 8 hourly during labour.
Q3 Q3 Regarding asthma in pregnancy, which of the following is false false....? A) If anaesthesia is required, regional blockade is preferred to GA due to the risk of some inhaled anaesthetic agents causing bronchospasm. C) Prostaglandin F2 should be used with extreme caution in women with asthma because of the risk of inducing bronchoconstriction. D) Continuous fetal monitoring is recommended for pregnant women presenting with acute severe asthma. E) Those taking > 5 mg/day of prednisolone for >2 weeks prior to delivery should receive hydrocortisone 100 mg IV 6 8 hourly during labour. - FALSE (it is those receiving >7.5mg/day)
Ref: BTS/SIGN Asthma Guideline Asthma Quick Reference Guide, July 2019, pg 23
Q4 Q4 Regarding diagnostic tests for asthma, which of the following is false false..... A) In adults with obstructive spirometry, an improvement in FEV1 of 12% in response to either 2 agonists or corticosteroid treatment trials, together with an increase in volume of 200 ml, is regarded as a positive test. B) Wheeze heard by a healthcare professional on auscultation increases the probability of asthma. C) When doing 'best of 3' peak flows (PEF), further blows should be done if the largest two PEF are not within 40 L/min of each other. D) PEF should be measured at least 2x/day if occupational asthma is suspected.
Q4 Q4 Regarding diagnostic tests for asthma, which of the following is false false..... A) In adults with obstructive spirometry, an improvement in FEV1 of 12% in response to either 2 agonists or corticosteroid treatment trials, together with an increase in volume of 200 ml, is regarded as a positive test. B) Wheeze heard by a healthcare professional on auscultation increases the probability of asthma. C) When doing 'best of 3' peak flows (PEF), further blows should be done if the largest two PEF are not within 40 L/min of each other. D) PEF should be measured at least 2x/day if occupational asthma is suspected. - FALSE (should be 4x/day)
Q5 Q5 Regarding 'direct challenge tests', which of the following is false false? A) A Provocation Concentration (PC) of 8 mg/ml or less is regarded as positive. B) The provocative concentration (PC) or dose (PD) is the dose of bronchoconstrictor required to cause a 10% fall in FEV1. C) Two thirds, or more, of adults with a positive methacholine challenge have asthma. D) The false negative rate is less than 10%.
Q5 Q5 Regarding 'direct challenge tests', which of the following is false false? A) A Provocation Concentration (PC) of 8 mg/ml or less is regarded as positive. B) The provocative concentration (PC) or dose (PD) is the dose of bronchoconstrictor required to cause a 10% fall in FEV1. - FALSE C) Two thirds, or more, of adults with a positive methacholine challenge have asthma. D) The false negative rate is less than 10%. Ref: BTS/SIGN Guidelines for the management of Asthma , July 2019, pg 14
Direct challenge tests Direct challenge tests A measure of airway responsiveness. Usually use methacholine or histamine. The provocative concentration (PC20) or dose (PD20) of bronchoconstrictor required to cause a 20% fall in FEV1.
Q6 Regarding Fractional exhaled nitric oxide (FeNO) levels, which of the following are false false? A) FeNo levels are increased in men. B) FeNo levels are reduced in cigarette smokers. C) FeNo levels are reduced by inhaled or oral steroids. D) FeNo levels are increased in allergic rhinitis. E) In steroid-naive adults, a FeNO level of 40 parts per billion (ppb) or more is regarded as positive. F) A negative test excludes asthma
Q6 Regarding Fractional exhaled nitric oxide (FeNO) levels, which of the following are false false? A) FeNo levels are increased in men. B) FeNo levels are reduced in cigarette smokers. C) FeNo levels are reduced by inhaled or oral steroids. D) FeNo levels are increased in allergic rhinitis. E) In steroid-naive adults, a FeNO level of 40 parts per billion (ppb) or more is regarded as positive. F) A negative test excludes asthma - FALSE
Fractional exhaled nitric oxide Fractional exhaled nitric oxide ( (FeNO FeNO) Testing ) Testing Can be used to find evidence of eosinophilic inflammation. A positive test increases the probability of asthma. A negative test does not exclude asthma. In steroid-naive adults, a FeNO level of 40 parts per billion (ppb) or more is regarded as positive.
Ref: BTS/SIGN Guideline for the Management of Asthma, July 2019, pg 15
Q7 Q7 38yr old pregnant woman presents to A&E with 2 days of wheeze and increased SOB. Two hours after treatment with nebulisers and steroids her RR is 18, Sats 95% on air, HR 84, BP 120/70. PEFR is 320L/min but she states that she does not feel better. Her 'best' recorded PEF is 400L/min. Which of the following is not is not a reason to consider hospital admission? A) A history of poor compliance with treatment. B) Presentation at night. C) Asthma attack despite adequate dose of oral corticosteroid prior to presentation. D) She still has significant symptoms E) Her PEFR post-treatment. F) Pregnancy.
Q7 Q7 38yr old pregnant woman presents to A&E with 2 days of wheeze and increased SOB. Two hours after treatment with nebulisers and steroids her RR is 18, Sats 95% on air, HR 84, BP 120/70. PEFR is 320 but she states that she does not feel better. Her 'best' recorded PEF is 400. Which of the following is not is not a reason to consider hospital admission? A) A history of poor compliance with treatment. B) Presentation at night. C) Asthma attack despite adequate dose of oral corticosteroid prior to presentation. D) She still has significant symptoms E) Her PEFR post-treatment. (which is 80% of 'best') F) Pregnancy.
Criteria for admission Criteria for admission
Q8 Regarding treatment of asthma with Omalizumab, which of the following is false? false? A) Omalizumab can be used to treat severe persistent confirmed allergic IgE-mediated asthma. B) It is used in those with continuous or frequent oral corticosteroid use, defined as >2 courses in the previous year. C) Patients must have stopped smoking. D) The dosage is determined by the concentration of serum IgE before the start of treatment and body weight. E) Response should be evaluated at 16wks, and treatment should be stopped if there is no improvement.
Q8 Regarding treatment of asthma with Omalizumab, which of the following is incorrect? incorrect? A) Omalizumab can be used to treat severe persistent confirmed allergic IgE-mediated asthma. B) It is used in those with continuous or frequent oral corticosteroid use, defined as >2 courses in the previous year. - Incorrect. C) Patients must have stopped smoking. D)The dosage is determined by the concentration of serum IgE before the start of treatment and body weight. E) Response should be evaluated at 16wks, and treatment should be stopped if there is no improvement.
NICE Guidance on Omalizumab 1.1 Omalizumab is recommended as an option for treating severe persistent confirmed allergic IgE-mediated asthma as an add-on to optimised standard therapy: who need continuous or frequent treatment with oral corticosteroids (defined as 4 or more courses in the previous year) 1.2 Optimised standard therapy is defined as a full trial of and, if tolerated, documented compliance with: inhaled high-dose corticosteroids long-acting beta2agonists leukotriene receptor antagonists theophyllines oral corticosteroids smoking cessation if clinically appropriate Ref: Omalizumab for treating severe persistent allergic asthma. NICE Technology appraisal guidance [TA278] April 2013