Treatment of HCV Genotype 1 Non-Cirrhotic Patients with Next Generation NS3/4A Protease Inhibitor and NS5A Inhibitor
Study on the effectiveness of ABT-493 and ABT-530 in treating HCV Genotype 1 patients who are treatment-naive or have failed previous treatment. Presented at the 66th Annual Meeting of the American Association for the Study of Liver Diseases.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
SURVEYOR-I: 98% 100% SVR4 in HCV Genotype 1 Non-Cirrhotic Treatment-Na ve or Pegylated Interferon/Ribavirin Null-Responders with the Combination of the Next Generation NS3/4A Protease Inhibitor ABT-493 and NS5A Inhibitor ABT-530 Fred Poordad,1Franco Felizarta,2Armen Asatryan,3Tarek Hassanein,4 Humberto Aguilar,5Jacob Lalezari,6J. Scott Overcash,7Teresa I. Ng,3 Ran Liu,3Chih-Wei Lin,3Federico J. Mensa,3Jens Kort3 1Texas Liver Institute, University of Texas Health Science Center, San Antonio, TX, USA; 2Private practice, Bakersfield, CA, USA; 3AbbVie Inc., North Chicago, IL, USA; 4Southern California GI and Liver Centers and Southern California Research Center, Coronado, CA, USA; 5Louisiana Research Center, Shreveport, LA, USA; 6Quest Clinical Research, San Francisco, CA, USA; 7eStudySite, San Diego, CA, USA 66th Annual Meeting of the American Association for the Study of Liver Diseases San Francisco, CA 15 November 2015 1
Disclosures F Poordad: Grant/Research support: Abbvie, Achillion Pharmaceuticals, Anadys Pharmaceuticals, Biolex Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, Genentech, Gilead Sciences, GlaxoSmithKline, GlobeImmune, Idenix Pharmaceuticals, Idera Pharmaceuticals, Intercept Pharmaceuticals, Janssen, Medarex, Medtronic, Merck, Novartis, Santaris Pharmaceuticals, Scynexis Pharmaceuticals, Vertex Pharmaceuticals, ZymoGenetics. Speaker: Gilead, Kadmon, Merck, Onyx/Bayer, Genentech, GlaxoSmithKline, Salix, Vertex. Consultant/Advisor: AbbVie, Achillion Pharmaceuticals, Anadys Pharmaceuticals, Biolex Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline, GlobeImmune, Idenix, Merck, Novartis, Tibotec/Janssen, Theravance, Vertex F Felizarta: Research support (principal investigator): AbbVie, Achillion, BMS, Gilead, Janssen, Merck, and Novartis. Speaker: AbbVie, Gilead, Janssen, Merck T Hassanein: Grants/Research support: AbbVie (Advisory Board), Boehringer-Ingelheim, Bristol-Myers Squibb (Advisory Board), Eisai, Gilead Sciences, Janssen, Idenix, Ikaria, Mochida, Roche, Ocera, Taigen, Takeda, Salix, Sundise, Vertex. Speaker: Baxter, Bristol-Myers Squibb, Gilead, Salix H Aguilar: Grants: AbbVie. Speaker: Santarus, Ironwood, AbbVie J Lalezari: Research support (principal investigator): AbbVie JS Overcash: No relevant conflicts to disclose A Asatryan, TI Ng, R Liu, CW Lin, F Mensa, and J Kort: AbbVie employees and may hold AbbVie stock or stock options. The design, study conduct, analysis, and financial support of the SURVEYOR-I (NCT02243280) study were provided by AbbVie. AbbVie participated in the interpretation of data, review, and approval of the content. All authors had access to all relevant data and participated in writing, review, and approval of this presentation. Medical writing support was provided by Sharanya Ford, PhD, of AbbVie. This presentation contains information on the investigational products ABT-493 and ABT-530. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 2
Next Generation Direct-Acting Antivirals ABT-493: pangenotypic HCV NS3/4A protease inhibitor* (EC50 0.9 2.8 nM) ABT-530: pangenotypic HCV NS5A inhibitor (EC50 1 4 pM) In vitro characteristics:1,2 Higher barrier to resistance Additive/synergistic antiviral activity Active against common variants eg, GT1 NS3: R155K, D168A/E/V eg, GT1 NS5A: M28T/V, Q30E/H/R, L31M/V, P32L, Y93C/H/N *ABT-493 identified by AbbVie and Enanta. 1. 2. Ng TI, et al. Abstract 636. 21st Conference on Retroviruses and Opportunistic Infections., Boston, 2014. Ng TI, et al. Abstract 639. 21st Conference on Retroviruses and Opportunistic Infections., Boston, 2014. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 3
Next Generation Direct-Acting Antivirals: ABT-493 ABT-493 demonstrates potent activity against major HCV genotypes in vitro Stable HCV Replicon EC50 (nM) GT1b GT2a 0.94 2.7a 0.21 5.3a 9.4 15 1.2 230 0.87 1.3 5.4 316 3.3 3.7 Protease Inhibitor GT1a 0.85 1.0 13 4.0 0.38 13 3.9 GT3a 1.6 19 472 1162 36 NA 6.1 GT4a 2.8 0.09 NA NA 1.2 NA 2.9 GT6a 0.86 0.68 NA NA 0.89 NA 1.5 ABT-493 Paritaprevir Simeprevir1,2 Asunaprevir3 Grazoprevir GS-94514 GS-98575 aStudy conducted at Southern Research Institute. NA, not available. 1. 2. 3. 4. 5. Simeprevir prescribing information Chase R, et al. IAPAC, 2013 McPhee F, et al. AAC, 2012 Yang H, et al. AAC, 2014 Taylor J, et al. EASL, 2015 SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 4
Next Generation Direct-Acting Antivirals: ABT-530 ABT-530 demonstrates potent pangenotypic activity against HCV in vitro Stable HCV Replicon EC50 (pM) GT2a GT2b 2a 2 12 4 13,000 NA 21,000 16,000 168,000 9 8 3 3000 1 4 21 ~150 24 NA NS5A Inhibitor GT1a 2 14 22 31 12 4 1 26 8 GT1b 4 5 3 4 15 3 2 5 3 GT3a 2 19 530 GT4a 2 2 13 390 9 3 2 NA 2 GT5a 1 3 5 150 75 1 1 NA 37 GT6a 3 366 74 1100 6 3 4 NA NA ABT-530 Ombitasvir Daclatasvir1 Ledipasvir2 Velpatasvir3 Elbasvir4 MK-84085 ACH-31026 IDX7197 12 20 2 NA 17 aStudy conducted at Southern Research Institute. NA, not available. 1. 2. 3. 4. Wang C, et al. AAC, 2014 Cheng G, et al. EASL, 2012; Harvoni prescribing information. Cheng G, et al. EASL, 2013 Liu R, et al. EASL, 2012 5. 6. 7. Asante-Appiah E, AASLD, 2014 Zhao Y, et al. EASL, 2012 Dousson C, et al. EASL, 2011 SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 5
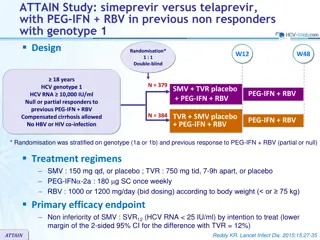
SURVEYOR-I Part 1: Study Design Day 1 Week 12 PT Week 24 Treatment period Post-treatment (PT) period ABT-493 200 mg + ABT-530 40 mg n=39 ABT-493 200 mg + ABT-530 120 mg n=40 Key Pharmacokinetics: Once-daily oral dosing Minimal metabolism and primary biliary excretion No renal excretion (<1%) ClinicalTrials.gov: NCT02243280. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 6
SURVEYOR-I Part 1: Key Eligibility Criteria and Endpoints Key inclusion criteria 18 to 70 years of age, inclusive HCV GT1 infection, HCV RNA >10,000 IU/mL HCV treatment-na ve or PegIFN/RBV null-responders Absence of cirrhosis Key exclusion criteria Previous use of any HCV DAAs ALT or AST >5x ULN, CrCl <50 ml/min, platelet count <120 109/L Herbal supplements and potent P-gp inducers were prohibited *Commonly prescribed concomitant medications (e.g., PPIs) were allowed Endpoints Efficacy: SVR12 (primary) and virologic failure Safety: adverse events (AEs) and laboratory abnormalities SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 7
SURVEYOR-I Part 1: Demographics and Patient Characteristics ABT-493 200 mg + ABT-530 40 mg (n = 39) 18 (46) 35 (90) 9 (23) 53 (30 70) 28 4.3 32 (82) 6.6 0.6 30 (77) ABT-493 200 mg + ABT-530 120 mg (n = 40) 23 (58) 34 (85) 7 (18) 52 (26 68) 28 5 31 (78) 6.7 0.6 34 (85) Male, n (%) White race, n (%) Hispanic or Latino ethnicity, n (%) Age, mean (range), years BMI, mean SD, kg/m2 IL28B non-CC genotype, n (%) HCV RNA, mean SD, log10 IU/mL HCV GT1a, n (%) Prior PegIFN/RBV experience, n (%) Na ve Null-responder Baseline fibrosis stage, n (%) F0 F1 F2 F3 25 (64) 14 (36) 25 (63) 15 (37) 27 (69) 5 (13) 7 (18)a 22 (55) 5 (13) 13 (32) aIncludes one patient with baseline F4 fibrosis stage. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 8
SURVEYOR-I Part 1: ITT SVR12 Rates 9 7 1 0 0 100 80 SV R 12, % Patients 60 40 20 38a 39 40 40 0 ABT-493 200 mg + ABT-530 120 mg 120 mg ABT-493 + ABT-530 200 mg + 40 mg 200 mg + aOne treatment-na ve patient with GT1a infection experienced virologic failure. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 9
SURVEYOR-I Part 1: ITT SVR12 Rates 9 7 1 0 0 100 80 SV R 12, % Patients 60 40 20 38a 39 40 40 0 ABT-493 + ABT-530 200 mg + 40 mg 200 mg + 120 mg aOne treatment-na ve patient with GT1a infection experienced relapse. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 10
SURVEYOR-I Part 1: ITT SVR12 Rates 9 7 1 0 0 100 100% (29/29) treatment-experienced patients achieved SVR12 80 SV R 12, % Patients 98% (49/50) treatment-na ve patients achieved SVR12 60 40 20 38a 39 40 40 0 ABT-493 + ABT-530 200 mg + 40 mg 200 mg + 120 mg aOne treatment-na ve patient with GT1a infection experienced relapse. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 11
SURVEYOR-I Part 1: Treatment Failure One patient in the low dose arm relapsed at post-treatment week 4 Patient Characteristics ABT-493 200 mg + ABT-530 40 mg 55 Male White F0 F1 1a C/C Na ve None NS5A: Q30K + H58D Treatment arm Age, years Gender Race Baseline fibrosis stage HCV subgenotype IL28B genotype Treatment experience Resistant variants at baseline Resistant variants at relapse SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 12
Amino Acid Variant Analysis by Population Sequencing 46 (58%) patients had baseline variants in NS3 and/or NS5A 100 Patients (%) 80 47% 60 40 8% 20 4% 0 NS3 only NS5A only NS3 and NS5A All patients with baseline NS3 and/or NS5A variantsa achieved SVR12 aBased on HCV Drug Resistance Working Group review of clinically relevant variants: Lontok E, et al. Hepatology. 2015; 62(3):715. NS3: 36, 43, 54, 55, 56, 80, 122, 155, 156, 168, and 170 NS5A: 28, 29, 30, 31, 32, 58, 92, and 93 SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 13
100% SVR12 in Patients with Baseline Variants Amino Acid Variant Analysis by Population Sequencing Genotype Baseline Variant T54S T54S, R155K, I170V V55A V55A, Q80K V55A, Q80K, S122G Q80K Q80K, I170V S122G R155K I170V V36I, S122N S122G S122N S122T M28V M28V, Q30H Q30H L31M Q30H, Y93H Y93H Number of Patients (N=79) 1 1 2 1 1 21 3 1 1 3 1 1 2 1 2 1 1 3 1 1 Viral Target 1a NS3 1b 1a NS5A 1b SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 14
SURVEYOR-I Part 1: Summary of Adverse Events ABT-493 200 mg + ABT-530 40 mg (n = 39) 30 (77) 0 1 (3)a 0 0 ABT-493 200 mg + ABT-530 120 mg (n = 40) 26 (65) 0 2 (5)b,c 1 (3)c 0 Event, n (%) Any AE AEs leading to study discontinuation Any Grade 3 (severe) AE Any serious AE Deaths AEs in >10% of patients Fatigue Headache Nausea 5 (13) 8 (21) 8 (21) 9 (23) 5 (13) 5 (13) AEs were graded per National Cancer Institute s Common Terminology Criteria for Adverse Events (CTCAE). aOne patient experienced a decrease in blood phosphorus deemed related to study drugs. bOnepatient experienced elevated blood glucose levels deemed not related to study drugs. cA serious Grade 3 AE of metastatic prostate cancer was deemed not related to study drugs and had onset after completion of study treatment. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 15
SURVEYOR-I Part 1: Laboratory Abnormalities ABT-493 200 mg + ABT-530 40 mg (n = 39) ABT-493 200 mg + ABT-530 120 mg (n = 40) Event, n (%) ALT Grade 2+ (>3 x ULN) AST Grade 2+ (>3 x ULN) Alkaline phosphatase Grade 2+ (>2.5 x ULN) Total bilirubin Grade 2+(>1.5 x ULN) Hemoglobin Grade 2 (<10 8 g/dL) Grade 3 (<8 g/dL) Presented are laboratory elevations that were increased levels from baseline. 0 0 0 0 0 0 0 0 0 0 1 (3) 0 SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 16
SURVEYOR-I Part 1: Summary 12-week dose-ranging study in non-cirrhotic patients with GT1 showed high SVR12 rates with once-daily ABT-493 + ABT-530 All but one patient achieved SVR12 This patient was treated with the lower ABT-530 40 mg dose and experienced relapse All patients with baseline NS3 and/or NS5A variants achieved SVR12 AEs were mostly mild in severity SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 17
SURVEYOR-I Part 1: Conclusions Up to 100% SVR12 achieved with ABT-493 + ABT-530 The combination was well tolerated Based on these results and data in other genotypes, the selected doses moving forward are: ABT-493: 300 mg QD ABT-530: 120 mg QD The SURVEYOR-I study has been expanded to assess: Patients without cirrhosis (8-week treatment) Patients with compensated cirrhosis (12-week treatment) SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 18
Acknowledgments The authors would like to express their gratitude to the patients and their families, investigators, study coordinators, and AbbVie/CRO study staff who made this study possible. SURVEYOR-I: ABT-493 and ABT-530 for HCV Genotype 1 Infection | AASLD | 15 November 2015 19